Department of Public Health and Infectious Diseases, "Sapienza" University of Rome, Viale del Policlinico 155, 00161 Rome, Italy.
J Neurovirol. 2013 Jun;19(3):274-9. doi: 10.1007/s13365-013-0167-9. Epub 2013 May 29.
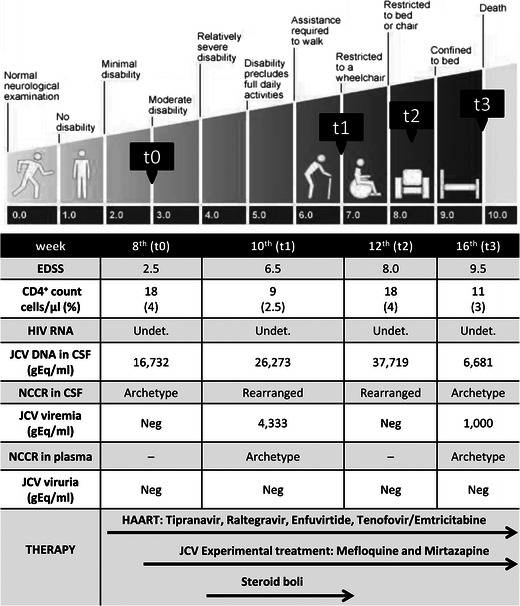
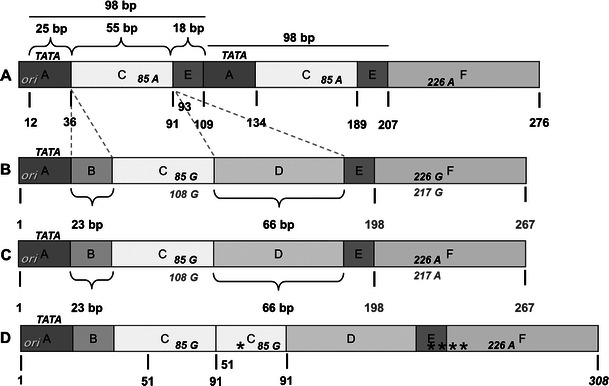
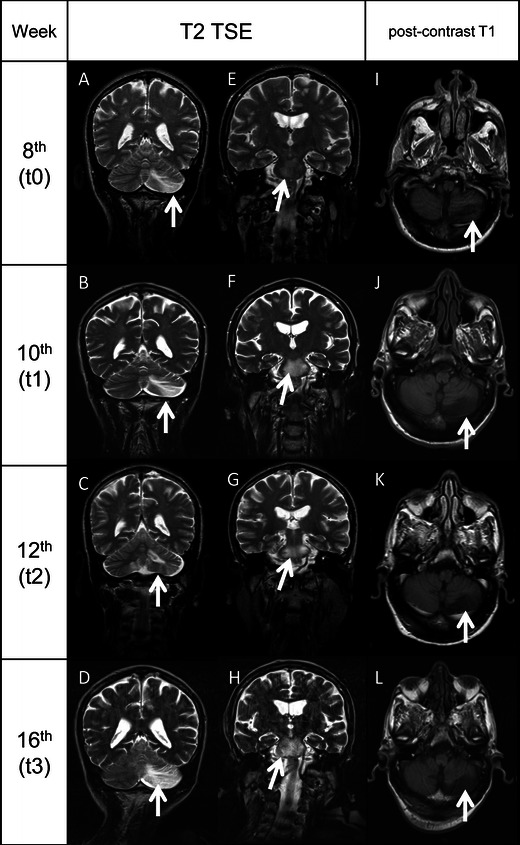
John Cunningham virus (JCV), the etiological agent of progressive multifocal leukoencephalopathy (PML), contains a hyper-variable non-coding control region usually detected in urine of healthy individuals as archetype form and in the brain and cerebrospinal fluid (CSF) of PML patients as rearranged form. We report a case of HIV-related PML with clinical, immunological and virological data longitudinally collected. On admission (t0), after 8-week treatment with a rescue highly active antiretroviral therapy (HAART), the patient showed a CSF-JCV load of 16,732 gEq/ml, undetectable HIV-RNA and an increase of CD4+ cell count. Brain magnetic resonance imaging (MRI) showed PML-compatible lesions without contrast enhancement. We considered PML-immune reconstitution inflammatory syndrome as plausible because of the sudden onset of neurological symptoms after the effective HAART. An experimental JCV treatment with mefloquine and mirtazapine was added to steroid boli. Two weeks later (t1), motor function worsened and MRI showed expanded lesions with cytotoxic oedema. CSF JCV-DNA increased (26,263 gEq/ml) and JCV viremia was detected. After 4 weeks (t2), JCV was detected only in CSF (37,719 gEq/ml), and 8 weeks after admission (t3), JC viral load decreased in CSF and JCV viremia reappeared. The patient showed high level of immune activation both in peripheral blood and CSF. He died 4 weeks later. Considering disease progression, combined therapy failure and immune hyper-activation, we finally classified the case as classical PML. The archetype variant found in CSF at t0/t3 and a rearranged sequence detected at t1/t2 suggest that PML can develop from an archetype virus and that the appearance of rearranged genotypes contribute to faster disease progression.
约翰·坎宁安病毒(JCV)是进行性多灶性白质脑病(PML)的病原体,其含有一个高度变异的非编码控制区,通常在健康个体的尿液中以原型形式检测到,而在 PML 患者的大脑和脑脊液(CSF)中则以重排形式检测到。我们报告了一例 HIV 相关的 PML,其临床、免疫学和病毒学数据进行了纵向采集。入院时(t0),在接受 8 周的挽救性高效抗逆转录病毒治疗(HAART)后,患者的 CSF-JCV 载量为 16,732 gEq/ml,HIV-RNA 不可检测,CD4+细胞计数增加。脑磁共振成像(MRI)显示符合 PML 的病变,无对比增强。我们认为 PML-免疫重建炎症综合征是合理的,因为在有效的 HAART 后突然出现了神经症状。由于类固醇冲击治疗后,患者的运动功能恶化,MRI 显示病变扩大伴有细胞毒性水肿,因此我们考虑加用了洛美沙星和米氮平实验性治疗 JCV。两周后(t1),病情恶化,MRI 显示病变扩大且伴有细胞毒性水肿。CSF JCV-DNA 增加(26,263 gEq/ml),并检测到 JCV 血症。4 周后(t2),仅在 CSF 中检测到 JCV(37,719 gEq/ml),入院后 8 周(t3),CSF 中的 JCV 载量下降,JCV 血症再次出现。患者外周血和 CSF 中均存在高水平的免疫激活。4 周后,患者死亡。考虑到疾病进展、联合治疗失败和免疫过度激活,我们最终将该病例归类为经典 PML。t0/t3 时 CSF 中发现的原型变体和 t1/t2 时检测到的重排序列提示,PML 可由原型病毒发展而来,重排基因型的出现可能导致疾病更快进展。