Division of General Pediatrics and Adolescent Medicine, Department of Pediatrics, Johns Hopkins University School of Medicine Baltimore, MD, USA.
Front Physiol. 2013 May 16;4:115. doi: 10.3389/fphys.2013.00115. eCollection 2013.
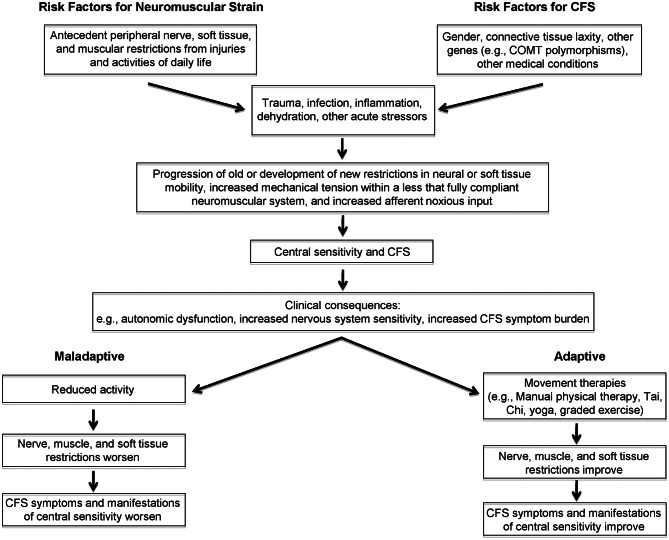
Individuals with chronic fatigue syndrome (CFS) have heightened sensitivity and increased symptoms following various physiologic challenges, such as orthostatic stress, physical exercise, and cognitive challenges. Similar heightened sensitivity to the same stressors in fibromyalgia (FM) has led investigators to propose that these findings reflect a state of central sensitivity. A large body of evidence supports the concept of central sensitivity in FM. A more modest literature provides partial support for this model in CFS, particularly with regard to pain. Nonetheless, fatigue and cognitive dysfunction have not been explained by the central sensitivity data thus far. Peripheral factors have attracted attention recently as contributors to central sensitivity. Work by Brieg, Sunderland, and others has emphasized the ability of the nervous system to undergo accommodative changes in length in response to the range of limb and trunk movements carried out during daily activity. If that ability to elongate is impaired-due to movement restrictions in tissues adjacent to nerves, or due to swelling or adhesions within the nerve itself-the result is an increase in mechanical tension within the nerve. This adverse neural tension, also termed neurodynamic dysfunction, is thought to contribute to pain and other symptoms through a variety of mechanisms. These include mechanical sensitization and altered nociceptive signaling, altered proprioception, adverse patterns of muscle recruitment and force of muscle contraction, reduced intra-neural blood flow, and release of inflammatory neuropeptides. Because it is not possible to differentiate completely between adverse neural tension and strain in muscles, fascia, and other soft tissues, we use the more general term "neuromuscular strain." In our clinical work, we have found that neuromuscular restrictions are common in CFS, and that many symptoms of CFS can be reproduced by selectively adding neuromuscular strain during the examination. In this paper we submit that neuromuscular strain is a previously unappreciated peripheral source of sensitizing input to the nervous system, and that it contributes to the pathogenesis of CFS symptoms, including cognitive dysfunction.
慢性疲劳综合征(CFS)患者在经历各种生理挑战后,如直立性应激、体力活动和认知挑战,会出现敏感性增加和症状加重。纤维肌痛(FM)中对相同应激源的类似敏感性增加,导致研究人员提出这些发现反映了中枢敏感性状态。大量证据支持 FM 中的中枢敏感性概念。更多的证据部分支持 CFS 中的这种模型,特别是在疼痛方面。然而,到目前为止,疲劳和认知功能障碍还不能用中枢敏感性数据来解释。外周因素最近引起了人们对中枢敏感性的关注。Brieg、Sunderland 等人的工作强调了神经系统在应对日常活动中肢体和躯干运动范围时,具有适应长度变化的能力。如果这种伸长能力受损-由于紧邻神经的组织的运动受限,或由于神经本身内的肿胀或粘连-则结果是神经内的机械张力增加。这种不利的神经张力,也称为神经动力学功能障碍,通过多种机制被认为会导致疼痛和其他症状。这些机制包括机械致敏和伤害性信号改变、本体感觉改变、肌肉募集和肌肉收缩力的不良模式、神经内血流减少以及炎症神经肽的释放。由于完全区分神经张力和肌肉、筋膜和其他软组织中的张力是不可能的,因此我们使用更通用的术语“神经肌肉紧张”。在我们的临床工作中,我们发现 CFS 中神经肌肉限制很常见,并且通过在检查期间选择性添加神经肌肉紧张,可以再现 CFS 的许多症状。在本文中,我们提出神经肌肉紧张是对神经系统的先前未被认识的外周致敏输入源,它有助于 CFS 症状的发病机制,包括认知功能障碍。