Department of Oncology, University Hospitals of Leicester NHS Trust, Leicester, UK.
BMJ Open. 2013 Jun 20;3(6):e002650. doi: 10.1136/bmjopen-2013-002650.
This cross-sectional survey investigated whether there were ethnic differences in depressive symptoms among British South Asian (BSA) patients with cancer compared with British White (BW) patients during 9 months following presentation at a UK Cancer Centre. We examined associations between depressed mood, coping strategies and the burden of symptoms.
Questionnaires were administered to 94 BSA and 185 BW recently diagnosed patients with cancer at baseline and at 3 and 9 months. In total, 53.8% of the BSA samples were born in the Indian subcontinent, 33% in Africa and 12.9% in the UK. Three screening tools for depression were used to counter concerns about ethnic bias and validity in linguistic translation. The Hospital Anxiety and Depression Scale (HADS-D), Patient Health Questionnaire-9 (both validated in Gujarati), Emotion Thermometers (including the Distress Thermometer (DT), Mini-MAC and the newly developed Cancer Insight and Denial questionnaire (CIDQ) were completed.
Leicestershire Cancer Centre, UK.
94 BSA and 185 BW recently diagnosed patients with cancer.
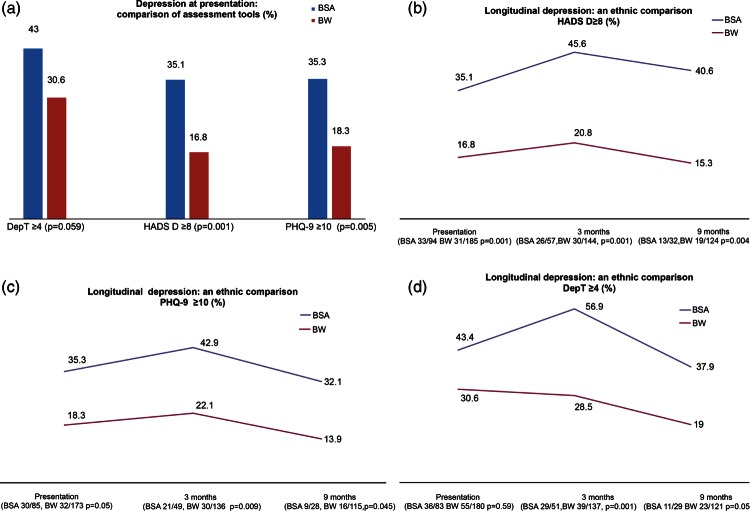
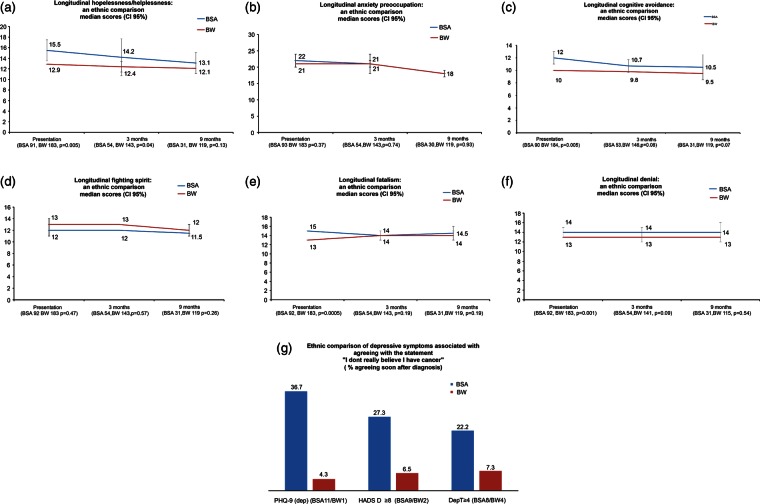
BSA self-reported significantly higher rates of depressive symptoms compared with BW patients longitudinally (HADS-D ≥8: baseline: BSA 35.1% vs BW 16.8%, p=0.001; 3 months BSA 45.6% vs BW 20.8%, p=0.001; 9 months BSA 40.6% vs BW 15.3%, p=0.004). BSA patients used potentially maladaptive coping strategies more frequently than BW patients at baseline (hopelessness/helplessness p=0.005, fatalism p=0.0005, avoidance p=0.005; the CIDQ denial statement 'I do not really believe I have cancer' p=0.0005). BSA patients experienced more physical symptoms (DT checklist), which correlated with ethnic differences in depressive symptoms especially at 3 months.
Health professionals need to be aware of a greater probability of depressive symptomatology (including somatic symptoms) and how this may present clinically in the first 9 months after diagnosis if this ethnic disparity in mental well-being is to be addressed.
本横断面调查旨在研究在英国癌症中心就诊 9 个月后,与英国白人(BW)患者相比,英国南亚裔(BSA)癌症患者的抑郁症状是否存在种族差异。我们研究了情绪低落、应对策略与症状负担之间的关系。
在基线时、3 个月和 9 个月时,共向 94 名 BSA 和 185 名 BW 新诊断癌症患者发放问卷。BSA 样本中,53.8%出生于印度次大陆,33%出生于非洲,12.9%出生于英国。使用三种抑郁筛查工具来应对语言翻译中的种族偏见和有效性问题。采用医院焦虑抑郁量表(HADS-D)、患者健康问卷-9(均在古吉拉特语中得到验证)、情绪温度计(包括痛苦温度计(DT)、Mini-MAC 和新开发的癌症洞察和否认问卷(CIDQ)进行评估。
英国莱斯特郡癌症中心。
94 名 BSA 和 185 名 BW 新诊断癌症患者。
BSA 自我报告的抑郁症状发生率显著高于 BW 患者,呈纵向趋势(HADS-D≥8:基线:BSA 35.1% vs BW 16.8%,p=0.001;3 个月:BSA 45.6% vs BW 20.8%,p=0.001;9 个月:BSA 40.6% vs BW 15.3%,p=0.004)。BSA 患者在基线时比 BW 患者更频繁地使用潜在的适应不良应对策略(绝望/无助,p=0.005;宿命论,p=0.0005;回避,p=0.005;CIDQ 否认声明“我真的不相信我得了癌症”,p=0.0005)。BSA 患者经历了更多的身体症状(DT 检查表),这与抑郁症状的种族差异相关,尤其是在 3 个月时。
如果要解决这种心理健康方面的种族差异,医务人员需要意识到在诊断后最初 9 个月内,患者出现抑郁症状(包括躯体症状)的可能性更大,以及这些症状在临床上的表现方式。