Authors' Affiliations: Departments of Environmental Health Science and Epidemiology, Johns Hopkins Bloomberg School of Public Health; Welch Center for Prevention, Epidemiology, and Clinical Research, Johns Hopkins University, Bloomberg School of Public Health; Departments of Medicine and Oncology, Johns Hopkins Medical Institutions, Baltimore; MedStar Health Research Institute, Hyattsville, Maryland; Georgetown-Howard Universities Center for Clinical and Translational Science, Washington, DC; Divison of Gynecology Oncology, Department of Obstetrics and Gynecology, Creighton University School of Medicine at St. Joseph's Hospital and Medical Center, Phoenix, Arizona; Missouri Breaks Industries Research Inc., Timber Lake, South Dakota; Environmental Epidemiology and Cancer Unit, National Center for Epidemiology, Carlos III Institute of Health; Consortium for Biomedical Research in Epidemiology & Public Health (CIBER en Epidemiología y Salud Pública - CIBERESP), Madrid, Spain; and Institute of Chemistry-Analytical Chemistry, Karl-Franzens University, Graz, Austria.
Cancer Epidemiol Biomarkers Prev. 2013 Nov;22(11):1944-53. doi: 10.1158/1055-9965.EPI-13-0234-T. Epub 2013 Oct 17.
Inorganic arsenic, a carcinogen at high exposure levels, is a major global health problem. Prospective studies on carcinogenic effects at low-moderate arsenic levels are lacking.
We evaluated the association between baseline arsenic exposure and cancer mortality in 3,932 American Indians, 45 to 74 years of age, from Arizona, Oklahoma, and North/South Dakota who participated in the Strong Heart Study from 1989 to 1991 and were followed through 2008. We estimated inorganic arsenic exposure as the sum of inorganic and methylated species in urine. Cancer deaths (386 overall, 78 lung, 34 liver, 18 prostate, 26 kidney, 24 esophagus/stomach, 25 pancreas, 32 colon/rectal, 26 breast, and 40 lymphatic/hematopoietic) were assessed by mortality surveillance reviews. We hypothesized an association with lung, liver, prostate, and kidney cancers.
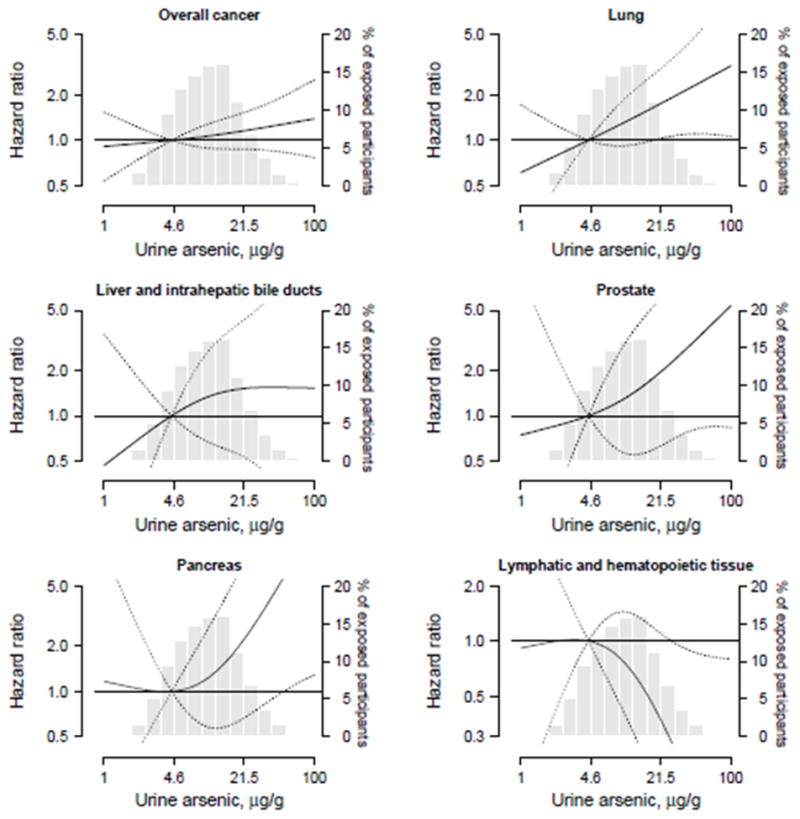
Median (interquartile range) urine concentration for inorganic plus methylated arsenic species was 9.7 (5.8-15.6) μg/g creatinine. The adjusted HRs [95% confidence interval (CI)] comparing the 80th versus 20th percentiles of arsenic were 1.14 (0.92-1.41) for overall cancer, 1.56 (1.02-2.39) for lung cancer, 1.34 (0.66, 2.72) for liver cancer, 3.30 (1.28-8.48) for prostate cancer, and 0.44 (0.14, 1.14) for kidney cancer. The corresponding hazard ratios were 2.46 (1.09-5.58) for pancreatic cancer, and 0.46 (0.22-0.96) for lymphatic and hematopoietic cancers. Arsenic was not associated with cancers of the esophagus and stomach, colon and rectum, and breast.
Low to moderate exposure to inorganic arsenic was prospectively associated with increased mortality for cancers of the lung, prostate, and pancreas.
These findings support the role of low-moderate arsenic exposure in development of lung, prostate, and pancreas cancer and can inform arsenic risk assessment.
无机砷是一种高暴露水平的致癌物质,是一个全球性的主要健康问题。低-中度砷暴露致癌作用的前瞻性研究尚缺乏。
我们评估了基线砷暴露与 3932 名年龄在 45 至 74 岁的美国印第安人癌症死亡率之间的关系,这些人来自亚利桑那州、俄克拉荷马州和北/南达科他州,他们于 1989 年至 1991 年参加了“强壮心脏研究”,并在 2008 年之前进行了随访。我们将尿液中的无机砷和甲基化砷的总和估计为无机砷的暴露量。通过死亡率监测审查评估癌症死亡(386 例总体死亡,78 例肺癌,34 例肝癌,18 例前列腺癌,26 例肾癌,24 例食管/胃癌,25 例胰腺癌,32 例结肠癌/直肠癌,26 例乳腺癌和 40 例淋巴/血液癌)。我们假设与肺癌、肝癌、前列腺癌和肾癌有关。
中位数(四分位距)尿无机加甲基砷浓度为 9.7(5.8-15.6)μg/g 肌酐。砷 80 百分位与 20 百分位相比,整体癌症的调整 HR[95%置信区间(CI)]为 1.14(0.92-1.41),肺癌为 1.56(1.02-2.39),肝癌为 1.34(0.66,2.72),前列腺癌为 3.30(1.28-8.48),肾癌为 0.44(0.14,1.14)。相应的危险比为胰腺癌为 2.46(1.09-5.58),淋巴和血液癌为 0.46(0.22-0.96)。砷与食管癌和胃癌、结肠癌和直肠癌以及乳腺癌无相关性。
低-中度无机砷暴露与肺癌、前列腺癌和胰腺癌的死亡率增加有关。
这些发现支持低-中度砷暴露在肺癌、前列腺癌和胰腺癌发展中的作用,并为砷风险评估提供信息。