Division of Tuberculosis Elimination, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention, Atlanta, Georgia.
Clin Infect Dis. 2013 Oct;57(8):1081-93. doi: 10.1093/cid/cit452. Epub 2013 Jul 9.
Pyrazinamide (PZA) is essential in tuberculosis treatment. We describe the prevalence, trends, and predictors of PZA resistance in Mycobacterium tuberculosis complex (MTBC) in the United States.
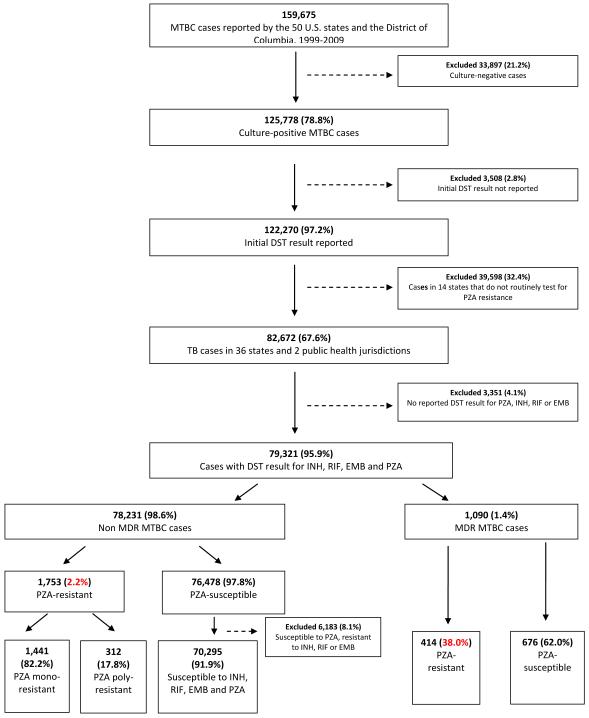
We analyzed culture-positive MTBC cases with reported drug susceptibility tests for PZA in 38 jurisdictions routinely testing for PZA susceptibility from 1999 to 2009. National Tuberculosis Genotyping Service data for 2004-2009 were used to distinguish M. tuberculosis from Mycobacterium bovis and determine phylogenetic lineage.
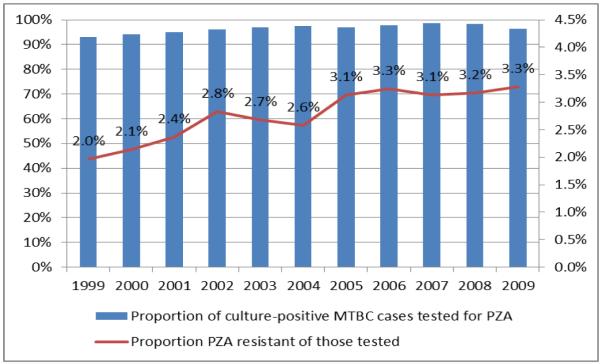
Overall 2.7% (2167/79 321) of MTBC cases had PZA resistance, increasing annually from 2.0% to 3.3% during 1999-2009 (P < .001), largely because of an increase in PZA monoresistance. PZA-monoresistant MTBC (vs drug-susceptible) was associated with an age of 0-24 years (adjusted prevalence ratio [aPR],1.50; 95% confidence interval [CI], 1.31-1.71), Hispanic ethnicity (aPR, 3.52; 95% CI, 2.96-4.18), human immunodeficiency virus infection (aPR, 1.43; 95% CI, 1.15-1.77), extrapulmonary disease (aPR, 3.02; 95% CI, 2.60-3.52), and normal chest radiograph (aPR, 1.88; 95% CI, 1.63-2.16) and was inversely associated with Asian (aPR, 0.59; 95% CI, .47-.73) and black (aPR, 0.37; 95% CI, .29-.49) race. Among multidrug-resistant (MDR) cases, 38.0% were PZA-resistant; PZA resistance in MDR MTBC was associated with female sex (aPR, 1.25; 95% CI, 1.08-1.46) and previous tuberculosis diagnosis (aPR, 1.37; 95% CI, 1.16-1.62). Of 28 080 cases with genotyping data, 925 (3.3%) had PZA resistance; 465 of 925 (50.3%) were M. bovis. In non-MDR M. tuberculosis cases, PZA resistance was higher in the Indo-Oceanic than the East Asian lineage (2.2% vs 0.9%, respectively; aPR, 2.26; 95% CI, 1.53-3.36), but in MDR cases it was lower in the Indo-Oceanic lineage (22.0% vs 43.4%, respectively; aPR, 0.54; 95% CI, .32-.90).
Specific human and mycobacterial characteristics were associated with PZA-resistant MTBC, reflecting both specific subgroups of the population and phylogenetic lineages of the mycobacteria.
吡嗪酰胺(PZA)是结核病治疗的重要药物。我们描述了美国结核分枝杆菌复合体(MTBC)中 PZA 耐药的流行率、趋势和预测因素。
我们分析了 1999 年至 2009 年 38 个常规进行 PZA 药敏试验的司法管辖区中报告了 PZA 药敏试验的培养阳性 MTBC 病例。2004-2009 年使用国家结核基因分型服务数据来区分结核分枝杆菌和牛分枝杆菌,并确定系统发育谱系。
总体而言,2.7%(79321 例中的 2167 例)的 MTBC 病例存在 PZA 耐药性,1999-2009 年期间耐药率逐年从 2.0%增加到 3.3%(P<0.001),主要是因为 PZA 单耐药性增加。与药敏 MTBC(vs 药物敏感)相比,PZA 单耐药 MTBC 与 0-24 岁年龄组(调整后的患病率比[aPR],1.50;95%置信区间[CI],1.31-1.71)、西班牙裔(aPR,3.52;95%CI,2.96-4.18)、人类免疫缺陷病毒感染(aPR,1.43;95%CI,1.15-1.77)、肺外疾病(aPR,3.02;95%CI,2.60-3.52)和正常胸片(aPR,1.88;95%CI,1.63-2.16)相关,与亚洲人(aPR,0.59;95%CI,0.47-0.73)和黑人(aPR,0.37;95%CI,0.29-0.49)种族呈负相关。在耐多药(MDR)病例中,38.0%为 PZA 耐药;MDR MTBC 中的 PZA 耐药与女性(aPR,1.25;95%CI,1.08-1.46)和既往结核病诊断(aPR,1.37;95%CI,1.16-1.62)相关。在有基因分型数据的 28080 例病例中,有 925 例(3.3%)存在 PZA 耐药;925 例中有 465 例(50.3%)为牛分枝杆菌。在非 MDR 结核分枝杆菌病例中,与东亚谱系相比,印度-印度洋谱系的 PZA 耐药率更高(分别为 2.2%和 0.9%;aPR,2.26;95%CI,1.53-3.36),但在 MDR 病例中,印度-印度洋谱系的 PZA 耐药率较低(分别为 22.0%和 43.4%;aPR,0.54;95%CI,0.32-0.90)。
特定的人类和分枝杆菌特征与 PZA 耐药性 MTBC 相关,这反映了人群的特定亚群和分枝杆菌的系统发育谱系。