García Patricia J, Cárcamo César P, Chiappe Marina, Valderrama Maria, La Rosa Sayda, Holmes King K, Mabey David C W, Peeling Rosanna W
Epidemiology, STD, and HIV Unit, School of Public Health and Administration Universidad Peruana Cayetano Heredia, Lima, Peru ; Department of Global Health, University of Washington, Seattle, Washington, United States of America.
PLoS One. 2013 Jun 26;8(6):e66905. doi: 10.1371/journal.pone.0066905. Print 2013.
Untreated maternal syphilis leads to adverse pregnancy outcomes. The use of point of care tests (POCT) offers an opportunity to improve screening coverage for syphilis and other aspects of health systems. Our objective is to present the experience of the introduction of POCT for syphilis in Peru and describe how new technology can catalyze health system strengthening.
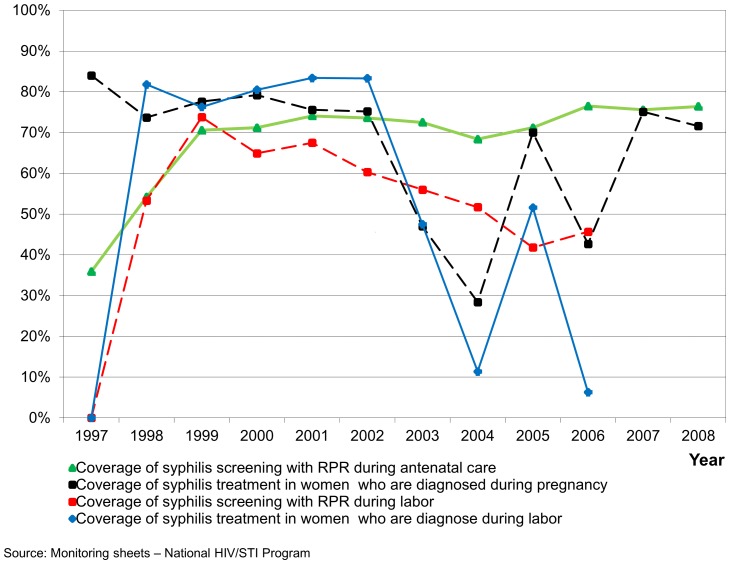
The study was implemented from September 2009-November 2010 to assess the feasibility of the use of a POCT for syphilis for screening pregnant women in Lima, Peru. Outcomes measured included access to syphilis screening, treatment coverage, partner treatment, effect on patient flow and service efficiency, acceptability among providers and patients, and sustainability.
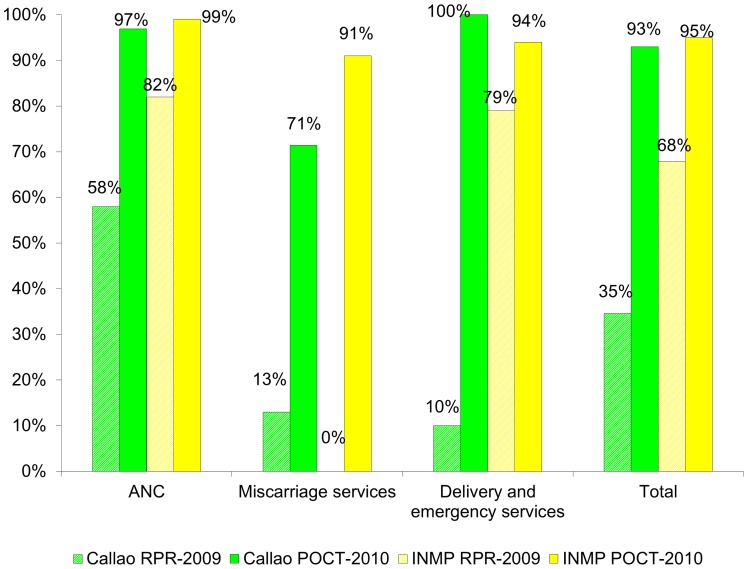
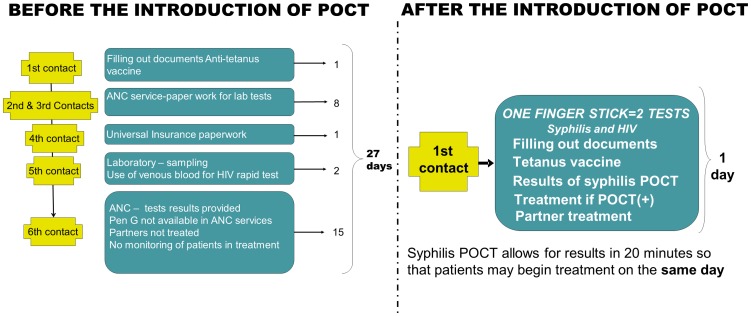
Before the introduction of POCT, a pregnant woman needed 6 visits to the health center in 27 days before she received her syphilis result. We trained 604 health providers and implemented the POCT for syphilis as the "two for one strategy", offering with one finger stick both syphilis and HIV testing. Implementation of the POCT resulted in testing and treatment on the first visit. Screening and treatment coverages for syphilis improved significantly compared with the previous year. Implementation of POCT has been scaled up nationally since the study ended, and coverages for screening, treatment and partner treatment have remained over 92%.
Implementation of POCT for syphilis proved feasible and acceptable, and led to improvement in several aspects of health services. For the process to be effective we highlight the importance of: (1) engaging the authorities; (2) dissipating tensions between providers and identifying champions; (3) training according to the needs; (4) providing monitoring, supervision, support and recognition; (5) sharing results and discussing actions together; (6) consulting and obtaining feedback from users; and (7) integrating with other services such as with rapid HIV testing.
未经治疗的孕产妇梅毒会导致不良妊娠结局。即时检验(POCT)的使用为提高梅毒筛查覆盖率及卫生系统的其他方面提供了契机。我们的目标是介绍秘鲁引入梅毒POCT的经验,并描述新技术如何促进卫生系统的强化。
该研究于2009年9月至2010年11月实施,以评估在秘鲁利马使用梅毒POCT筛查孕妇的可行性。测量的结果包括梅毒筛查的可及性、治疗覆盖率、性伴侣治疗、对患者流程和服务效率的影响、提供者和患者的可接受性以及可持续性。
在引入POCT之前,一名孕妇在收到梅毒检测结果前27天需要到卫生中心就诊6次。我们培训了604名卫生服务提供者,并实施了梅毒POCT的“二合一策略”,即通过一次指尖采血同时进行梅毒和艾滋病毒检测。POCT的实施使得在首次就诊时就能进行检测和治疗。与上一年相比,梅毒的筛查和治疗覆盖率显著提高。自研究结束后,POCT已在全国范围内扩大规模,筛查、治疗和性伴侣治疗的覆盖率一直保持在92%以上。
实施梅毒POCT被证明是可行且可接受的,并在卫生服务的几个方面带来了改善。为使该过程有效,我们强调以下几点的重要性:(1)与当局合作;(2)消除提供者之间的紧张关系并确定倡导者;(3)根据需求进行培训;(4)提供监测、监督、支持和认可;(5)共享结果并共同讨论行动;(6)咨询用户并获取反馈;(7)与其他服务(如快速艾滋病毒检测)整合。