Research Department of Infection and Population Health, University College London, London, United Kingdom.
PLoS One. 2013 Jul 10;8(7):e68152. doi: 10.1371/journal.pone.0068152. Print 2013.
Hepatitis B coinfection is common in HIV-positive individuals and as antiretroviral therapy has made death due to AIDS less common, hepatitis has become increasingly important. Several drugs are available to treat hepatitis B. The most potent and the one with the lowest risk of resistance appears to be tenofovir (TDF). However there are several questions that remain unanswered regarding the use of TDF, including the proportion of patients that achieves suppression of HBV viral load and over what time, whether suppression is durable and whether prior treatment with other HBV-active drugs such as lamivudine, compromises the efficacy of TDF due to possible selection of resistant HBV strains.
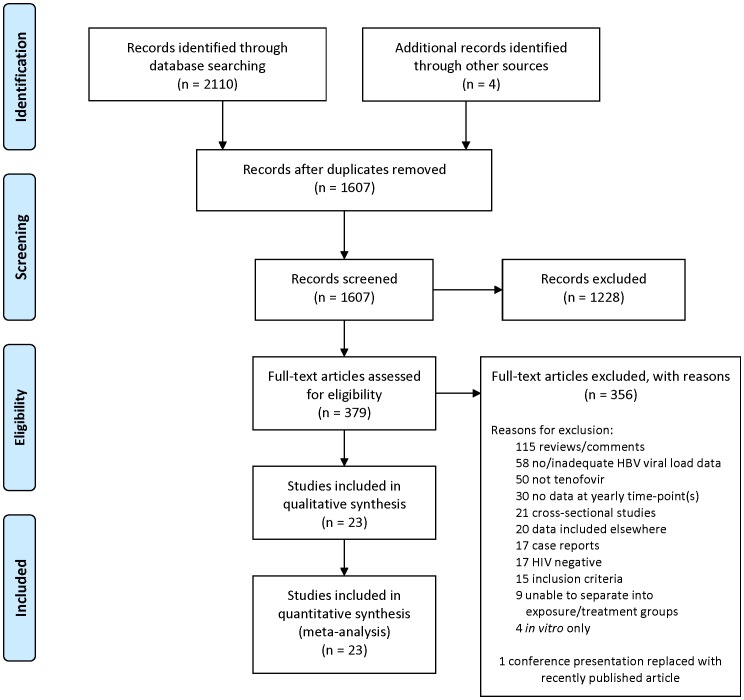
A systematic review and meta-analysis following PRISMA guidelines and using multilevel mixed effects logistic regression, stratified by prior and/or concomitant use of lamivudine and/or emtricitabine.
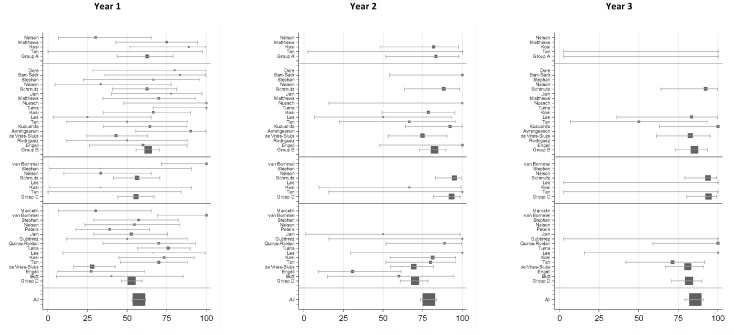
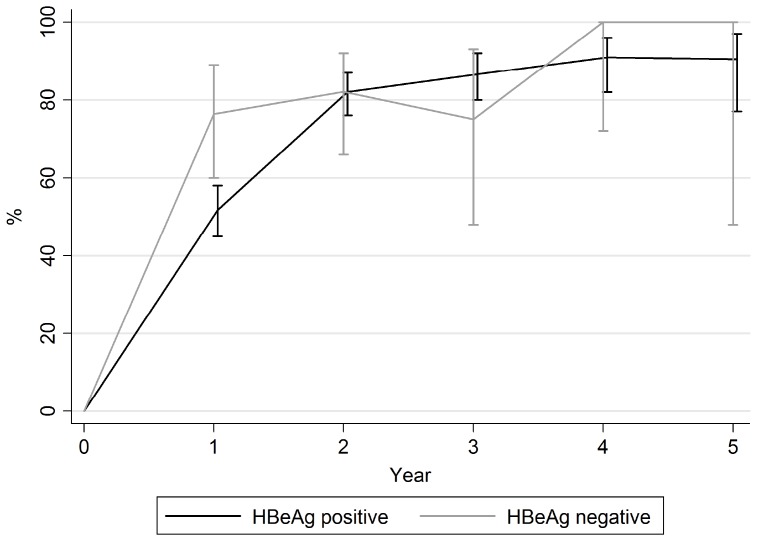
Data was available from 23 studies including 550 HBV/HIV coinfected patients treated with TDF. Follow up was for up to seven years but to ensure sufficient power the data analyses were limited to three years. The overall proportion achieving suppression of HBV replication was 57.4%, 79.0% and 85.6% at one, two and three years, respectively. No effect of prior or concomitant 3TC/FTC was shown. Virological rebound on TDF treatment was rare.
TDF suppresses HBV to undetectable levels in the majority of HBV/HIV coinfected patients with the proportion fully suppressed continuing to increase during continuous treatment. Prior treatment with 3TC/FTC does not compromise efficacy of TDF treatment. The use of combination treatment with 3TC/FTC offers no significant benefit over TDF alone.
乙型肝炎病毒(HBV)合并感染在 HIV 阳性个体中很常见,随着抗逆转录病毒疗法使艾滋病相关死亡变得罕见,HBV 感染变得越来越重要。有几种药物可用于治疗 HBV。其中最有效且耐药风险最低的似乎是替诺福韦(TDF)。然而,关于 TDF 的使用仍存在一些未解决的问题,包括达到 HBV 病毒载量抑制的患者比例以及达到抑制所需的时间、抑制是否持久以及先前使用拉米夫定等其他 HBV 活性药物是否会因可能选择耐药 HBV 株而影响 TDF 的疗效。
根据 PRISMA 指南进行系统评价和荟萃分析,并使用多水平混合效应逻辑回归,按先前和/或同时使用拉米夫定和/或恩曲他滨进行分层。
共有 23 项研究的数据可供使用,包括 550 例接受 TDF 治疗的 HBV/HIV 合并感染患者。随访时间长达七年,但为了确保有足够的效力,数据分析仅限于三年。在一年、两年和三年时,达到 HBV 复制抑制的总体比例分别为 57.4%、79.0%和 85.6%。先前或同时使用 3TC/FTC 没有显示出效果。TDF 治疗时发生病毒学反弹的情况很少见。
TDF 可使大多数 HBV/HIV 合并感染患者的 HBV 抑制到无法检测的水平,随着持续治疗,完全抑制的比例继续增加。先前使用 3TC/FTC 不会影响 TDF 治疗的疗效。与单独使用 TDF 相比,联合使用 3TC/FTC 并不能带来显著的益处。