Division of Gastroenterology, University of California Irvine, Irvine, CA, USA.
Hepatology. 2010 Sep;52(3):833-44. doi: 10.1002/hep.23744.
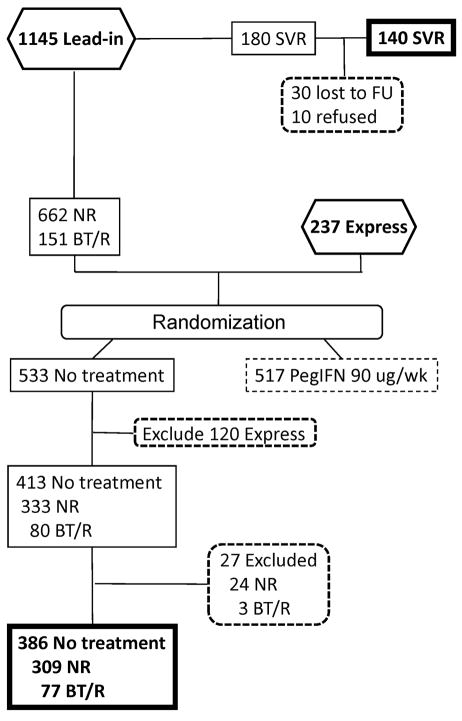
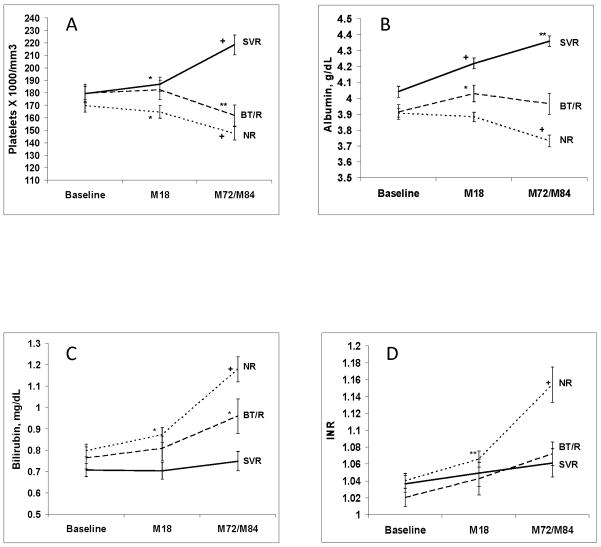
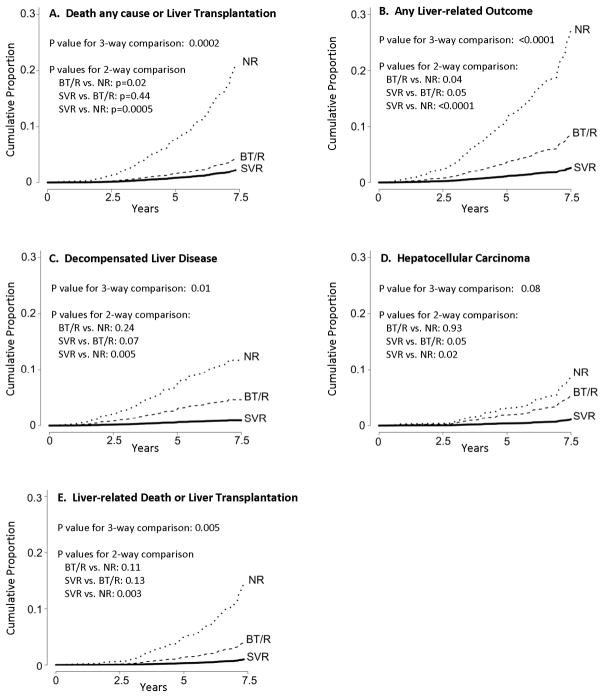
Retrospective studies suggest that subjects with chronic hepatitis C and advanced fibrosis who achieve a sustained virological response (SVR) have a lower risk of hepatic decompensation and hepatocellular carcinoma (HCC). In this prospective analysis, we compared the rate of death from any cause or liver transplantation, and of liver-related morbidity and mortality, after antiviral therapy among patients who achieved SVR, virologic nonresponders (NR), and those with initial viral clearance but subsequent breakthrough or relapse (BT/R) in the HALT-C (Hepatitis C Antiviral Long-Term Treatment Against Cirrhosis) Trial. Laboratory and/or clinical outcome data were available for 140 of the 180 patients who achieved SVR. Patients with nonresponse (NR; n = 309) or who experienced breakthrough or relapse (BT/R; n = 77) were evaluated every 3 months for 3.5 years and then every 6 months thereafter. Outcomes included death, liver-related death, liver transplantation, decompensated liver disease, and HCC. Median follow-up for the SVR, BT/R, and NR groups of patients was 86, 85, and 79 months, respectively. At 7.5 years, the adjusted cumulative rate of death/liver transplantation and of liver-related morbidity/mortality in the SVR group (2.2% and 2.7%, respectively) was significantly lower than that of the NR group (21.3% and 27.2%, P < 0.001 for both) but not the BT/R group (4.4% and 8.7%). The adjusted hazard ratio (HR) for time to death/liver transplantation (HR = 0.17, 95% confidence interval [CI] = 0.06-0.46) or development of liver-related morbidity/mortality (HR = 0.15, 95% CI = 0.06-0.38) or HCC (HR = 0.19, 95% CI = 0.04-0.80) was significant for SVR compared to NR. Laboratory tests related to liver disease severity improved following SVR.
Patients with advanced chronic hepatitis C who achieved SVR had a marked reduction in death/liver transplantation, and in liver-related morbidity/mortality, although they remain at risk for HCC.
回顾性研究表明,慢性丙型肝炎合并晚期纤维化的患者如果获得持续病毒学应答(SVR),其肝失代偿和肝细胞癌(HCC)的风险较低。在 HALT-C(丙型肝炎抗病毒长期治疗肝硬化)试验中,我们对达到 SVR、病毒学无应答(NR)和初始病毒清除但随后突破或复发(BT/R)的患者进行了抗病毒治疗后的任何原因或肝移植的死亡率、肝脏相关发病率和死亡率进行了前瞻性分析。180 名达到 SVR 的患者中有 140 名提供了实验室和/或临床结果数据。无应答(NR;n=309)或突破或复发(BT/R;n=77)的患者每 3 个月评估一次,共 3.5 年,此后每 6 个月评估一次。结果包括死亡、肝脏相关死亡、肝移植、失代偿性肝病和 HCC。SVR、BT/R 和 NR 组患者的中位随访时间分别为 86、85 和 79 个月。7.5 年后,SVR 组的死亡/肝移植和肝脏相关发病率/死亡率的累积率调整后分别为 2.2%和 2.7%,明显低于 NR 组(分别为 21.3%和 27.2%,P<0.001),但与 BT/R 组(分别为 4.4%和 8.7%)无差异。死亡/肝移植(HR=0.17,95%CI=0.06-0.46)或肝脏相关发病率/死亡率(HR=0.15,95%CI=0.06-0.38)或 HCC(HR=0.19,95%CI=0.04-0.80)的时间调整风险比(HR)对 SVR 与 NR 相比均有显著意义。SVR 后与肝脏疾病严重程度相关的实验室检查有所改善。
慢性丙型肝炎合并晚期纤维化的患者获得 SVR 后,死亡/肝移植以及肝脏相关发病率/死亡率显著降低,但仍有 HCC 风险。