Reginelli A, Genovese Ea, Cappabianca S, Iacobellis F, Berritto D, Fonio P, Coppolino F, Grassi R
Second University of Naples, Department of Clinical and Experimental Internistic F, Magrassi - A, Lanzara, Naples, Italy.
Crit Ultrasound J. 2013 Jul 15;5 Suppl 1(Suppl 1):S7. doi: 10.1186/2036-7902-5-S1-S7.
Intestinal ischemia is an abdominal emergency that accounts for approximately 2% of gastrointestinal illnesses. It represents a complex of diseases caused by impaired blood perfusion to the small and/or large bowel including acute arterial mesenteric ischemia (AAMI), acute venous mesenteric ischemia (AVMI), non occlusive mesenteric ischemia (NOMI), ischemia/reperfusion injury (I/R), ischemic colitis (IC). In this study different study methods (US, CT) will be correlated in the detection of mesenteric ischemia imaging findings due to various etiologies.
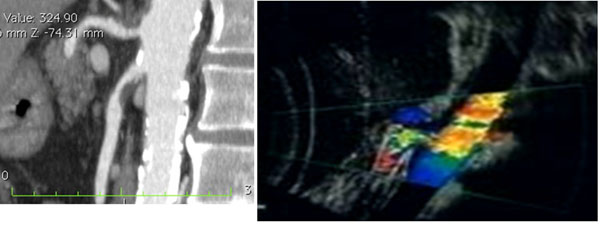
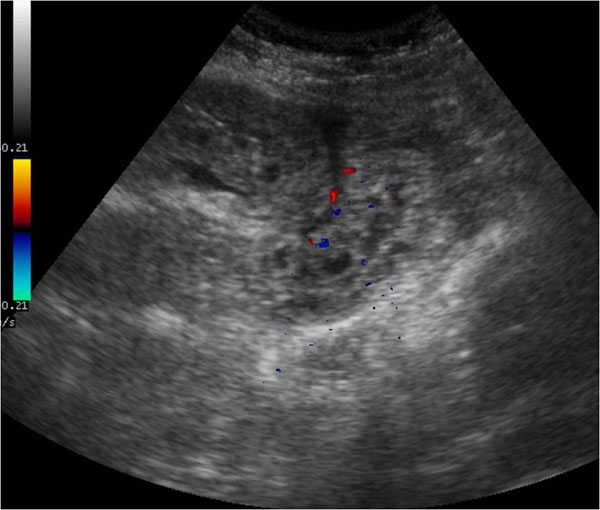
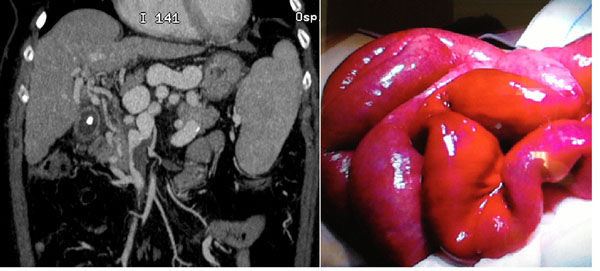
Basing on experience of our institutions, over 200 cases of mesenteric ischemia/infarction investigated with both US and CT were evaluated considering, in particular, the following findings: presence/absence of arterial/venous obstruction, bowel wall thickness and enhancement, presence/absence of spastic reflex ileus, hypotonic reflex ileus or paralitic ileus, mural and/or portal/mesenteric pneumatosis, abdominal free fluid, parenchymal ischemia/infarction (liver, kidney, spleen).
To make an early diagnosis useful to ensure a correct therapeutic approach, it is very important to differentiate between occlusive (arterial,venous) and nonocclusive causes (NOMI). The typical findings of each forms of mesenteric ischemia are explained in the text.
At present, the reference diagnostic modality for intestinal ischaemia is contrast-enhanced CT. However, there are some disadvantages associated with these techniques, such as radiation exposure, potential nephrotoxicity and the risk of an allergic reaction to the contrast agents. Thus, not all patients with suspected bowel ischaemia can be subjected to these examinations. Despite its limitations, US could constitutes a good imaging method as first examination in acute settings of suspected mesenteric ischemia.
肠缺血是一种腹部急症,约占胃肠道疾病的2%。它是由小肠和/或大肠血液灌注受损引起的一系列疾病,包括急性肠系膜动脉缺血(AAMI)、急性肠系膜静脉缺血(AVMI)、非闭塞性肠系膜缺血(NOMI)、缺血/再灌注损伤(I/R)、缺血性结肠炎(IC)。在本研究中,将对不同的研究方法(超声、CT)在检测各种病因引起的肠系膜缺血影像学表现方面的相关性进行研究。
根据我们机构的经验,对200多例同时接受超声和CT检查的肠系膜缺血/梗死病例进行评估,特别考虑以下表现:动脉/静脉阻塞的有无、肠壁厚度及强化情况、痉挛性反射性肠梗阻、低张性反射性肠梗阻或麻痹性肠梗阻的有无、肠壁和/或门静脉/肠系膜积气、腹腔游离液体、实质器官缺血/梗死(肝脏、肾脏、脾脏)。
为了做出有助于确保正确治疗方法的早期诊断,区分闭塞性(动脉、静脉)和非闭塞性病因(NOMI)非常重要。文中对每种肠系膜缺血形式的典型表现进行了解释。
目前,肠缺血的参考诊断方法是增强CT。然而,这些技术存在一些缺点,如辐射暴露、潜在的肾毒性以及对造影剂过敏反应的风险。因此,并非所有疑似肠缺血的患者都能接受这些检查。尽管存在局限性,但超声可作为疑似肠系膜缺血急性病例的首选检查方法,是一种很好的影像学检查手段。