Farid Shakil, Mohamed Shaza, Devbhandari Mohan, Kneale Matthew, Richardson Malcolm, Soon Sing Y, Jones Mark T, Krysiak Piotr, Shah Rajesh, Denning David W, Rammohan Kandadai
J Cardiothorac Surg. 2013 Aug 5;8:180. doi: 10.1186/1749-8090-8-180.
Surgery for pulmonary aspergillosis is infrequent and often challenging. Risk assessment is imprecise and new antifungals may ameliorate some surgical risks. We evaluated the medical and surgical management of these patients, including perioperative and postoperative antifungal therapy.
Retrospective study of patients who underwent surgery for pulmonary aspergillosis between September 1996 and September 2011.
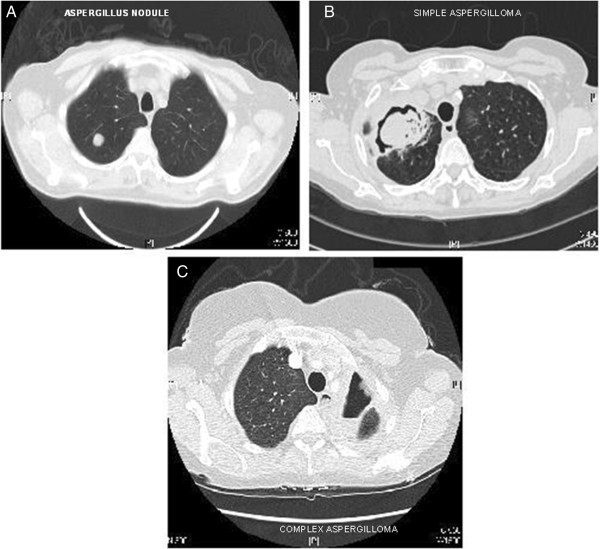
30 patients underwent surgery with 23 having a preoperative tissue diagnosis while 7 were confirmed post-resection. The median age was 57 years (17-78). The commonest presenting symptoms were cough (40%, n = 12) and haemoptysis (43%, n = 13). Twelve (40%) patients had simple aspergilloma (including 2 with Aspergillus nodules) while the remaining 18 (60%) had chronic cavitary pulmonary aspergillosis (CCPA) (complex aspergilloma). Most of the patients had underlying lung disease: tuberculosis (20%, n = 6), asthma (26%, n = 8) and COPD (20%, n = 6). The procedures included lobectomy 50% (n = 15), pneumonectomy 10% (n = 3), sublobar resection 27% (n = 8), decortication 7% (n = 2), segmentectomy 3% (n = 1), thoracoplasty 3% (n = 1), bullectomy and pleurectomy 3% (n = 1), 6% (n = 2) lung transplantation for associated disease. Median hospital stay was 9.5 days (3-37). There was no operative and 30 day mortality. Main complications were prolonged air leak (n = 7, 23%), empyema (n = 6, 20%), respiratory failure requiring tracheostomy /reintubation (n = 4, 13%). Recurrence of CCPA was noted in 8 patients (26%), most having prior CCPA (75%). Taurolidine 2% was active against all 9 A. fumigatus isolates and used for pleural decontamination during surgery.
Surgery in patients with chronic pulmonary aspergillosis offered good outcomes with an acceptable morbidity in a difficult clinical situation; recurrence is problematic.
肺曲霉病的手术治疗并不常见,且往往具有挑战性。风险评估不够精确,新型抗真菌药物可能会降低一些手术风险。我们评估了这些患者的内科和外科治疗,包括围手术期和术后抗真菌治疗。
对1996年9月至2011年9月期间接受肺曲霉病手术的患者进行回顾性研究。
30例患者接受了手术,其中23例术前有组织学诊断,7例术后确诊。中位年龄为57岁(17 - 78岁)。最常见的症状是咳嗽(40%,n = 12)和咯血(43%,n = 13)。12例(40%)患者患有单纯曲菌球(包括2例有曲霉结节),其余18例(60%)患有慢性空洞性肺曲霉病(CCPA)(复杂曲菌球)。大多数患者有基础肺部疾病:肺结核(20%,n = 6)、哮喘(26%,n = 8)和慢性阻塞性肺疾病(20%,n = 6)。手术方式包括肺叶切除术50%(n = 15)、全肺切除术10%(n = 3)、肺段以下切除术27%(n = 8)、胸膜剥脱术7%(n = 2)、肺段切除术3%(n = 1)、胸廓成形术3%(n = 1)、肺大疱切除术和胸膜切除术3%(n = 1)、因相关疾病进行肺移植6%(n = 2)。中位住院时间为9.5天(3 - 37天)。无手术及30天死亡率。主要并发症为持续性漏气(n = 7,23%)、脓胸(n = 6,20%)、需要气管切开/重新插管的呼吸衰竭(n = 4,13%)。8例(26%)患者出现CCPA复发,大多数患者既往有CCPA(75%)。2%的牛磺罗定对所有9株烟曲霉分离株均有活性,用于手术期间的胸膜去污。
慢性肺曲霉病患者的手术治疗在困难的临床情况下取得了良好的效果,发病率可接受;复发是个问题。