Corresponding author: Annabelle S. Slingerland,
Diabetes Care. 2013 Oct;36(10):3054-61. doi: 10.2337/dc12-1865. Epub 2013 Aug 15.
Diabetes treatment should be effective and cost-effective. HbA1c-associated complications are costly. Would patient-centered care be more (cost-) effective if it was targeted to patients within specific HbA1c ranges?
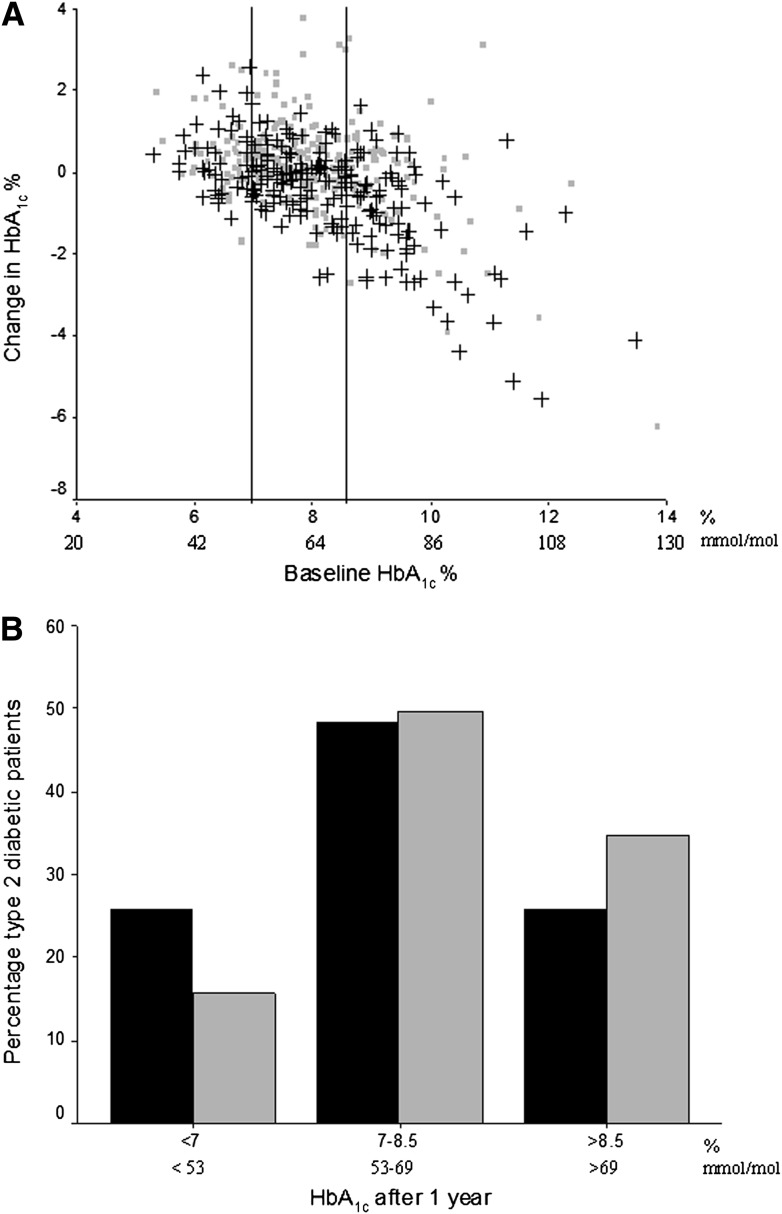
This prospective, cluster-randomized, controlled trial involved 13 hospitals (clusters) in the Netherlands and 506 patients with type 2 diabetes randomized to patient-centered (n=237) or usual care (controls) (n=269). Primary outcomes were change in HbA1c and quality-adjusted life years (QALYs); costs and incremental costs (USD) after 1 year were secondary outcomes. We applied nonparametric bootstrapping and probabilistic modeling over a lifetime using a validated Dutch model. The baseline HbA1c strata were <7.0% (53 mmol/mol), 7.0-8.5%, and >8.5% (69 mmol/mol).
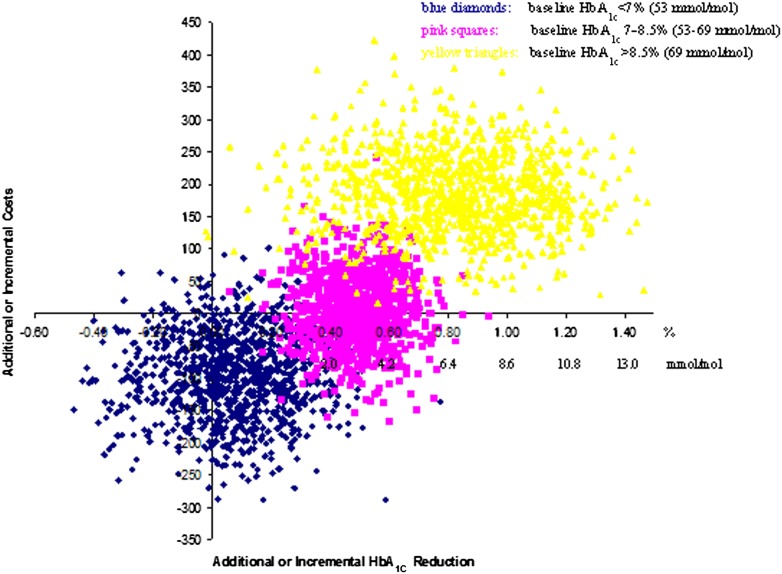
Patient-centered care was most effective and cost-effective in those with baseline HbA1c>8.5% (69 mmol/mol). After 1 year, the HbA1c reduction was 0.83% (95% CI 0.81-0.84%) (6.7 mmol/mol [6.5-6.8]), and the incremental cost-effectiveness ratio (ICER) was 261 USD (235-288) per QALY. Over a lifetime, 0.54 QALYs (0.30-0.78) were gained at a cost of 3,482 USD (2,706-4,258); ICER 6,443 USD/QALY (3,199-9,686). For baseline HbA1c 7.0-8.5% (53-69 mmol/mol), 0.24 QALY (0.07-0.41) was gained at a cost of 4,731 USD (4,259-5,205); ICER 20,086 USD (5,979-34,193). Care was not cost-effective for patients at a baseline HbA1c<7.0% (53 mmol/mol).
Patient-centered care is more valuable when targeted to patients with HbA1c>8.5% (69 mmol/mol), confirming clinical intuition. The findings support treatment in those with baseline HbA1c 7-8.5% (53-69 mmol/mol) and demonstrate little to no benefit among those with HbA1c<7% (53 mmol/mol). Further studies should assess different HbA1c strata and additional risk profiles to account for heterogeneity among patients.
糖尿病治疗应既有效又具成本效益。糖化血红蛋白相关并发症代价高昂。如果以特定糖化血红蛋白范围内的患者为目标,以患者为中心的护理是否会更具(成本)效益?
本前瞻性、整群随机对照试验纳入荷兰的 13 家医院(群组)和 506 名 2 型糖尿病患者,将患者随机分为以患者为中心(n=237)或常规护理(对照组)(n=269)。主要结局是糖化血红蛋白和质量调整生命年(QALY)的变化;次要结局是 1 年后的成本和增量成本(美元)。我们在一生中使用经过验证的荷兰模型进行了非参数引导和概率建模。基线糖化血红蛋白分层为<7.0%(53mmol/mol)、7.0-8.5%和>8.5%(69mmol/mol)。
以基线糖化血红蛋白>8.5%(69mmol/mol)的患者为目标,以患者为中心的护理最有效且最具成本效益。1 年后,糖化血红蛋白降低 0.83%(95%CI0.81-0.84%)(6.7mmol/mol[6.5-6.8]),增量成本效益比(ICER)为每 QALY 261 美元(235-288)。在一生中,以 3482 美元(2706-4258)的成本获得了 0.54 个 QALY(0.30-0.78);ICER为 6443 美元/QALY(3199-9686)。对于基线糖化血红蛋白为 7.0-8.5%(53-69mmol/mol),以 4731 美元(4259-5205)的成本获得了 0.24 个 QALY(0.07-0.41);ICER为 20086 美元(5979-34193)。对于基线糖化血红蛋白<7.0%(53mmol/mol)的患者,护理不具成本效益。
以基线糖化血红蛋白>8.5%(69mmol/mol)的患者为目标,以患者为中心的护理更有价值,证实了临床直觉。研究结果支持对基线糖化血红蛋白为 7-8.5%(53-69mmol/mol)的患者进行治疗,并表明糖化血红蛋白<7%(53mmol/mol)的患者获益甚微。需要进一步研究来评估不同的糖化血红蛋白分层和其他风险概况,以解释患者之间的异质性。