Pope Janet E, Haraoui Boulos, Thorne J Carter, Vieira Andrew, Poulin-Costello Melanie, Keystone Edward C
Division of Rheumatology, Department of Medicine, The University of Western Ontario, St Joseph's Health Centre, London, Ontario, Canada.
Department of Rheumatology, Centre Hospitalier de l'Université de Montréal, Montreal, Quebec, Canada.
Ann Rheum Dis. 2014 Dec;73(12):2144-51. doi: 10.1136/annrheumdis-2013-203684. Epub 2013 Aug 26.
To determine if withdrawing methotrexate (MTX) after 6 months of combination etanercept (ETN)+MTX, in MTX-inadequate responders with active rheumatoid arthritis (RA), is non-inferior to continuing ETN+MTX.
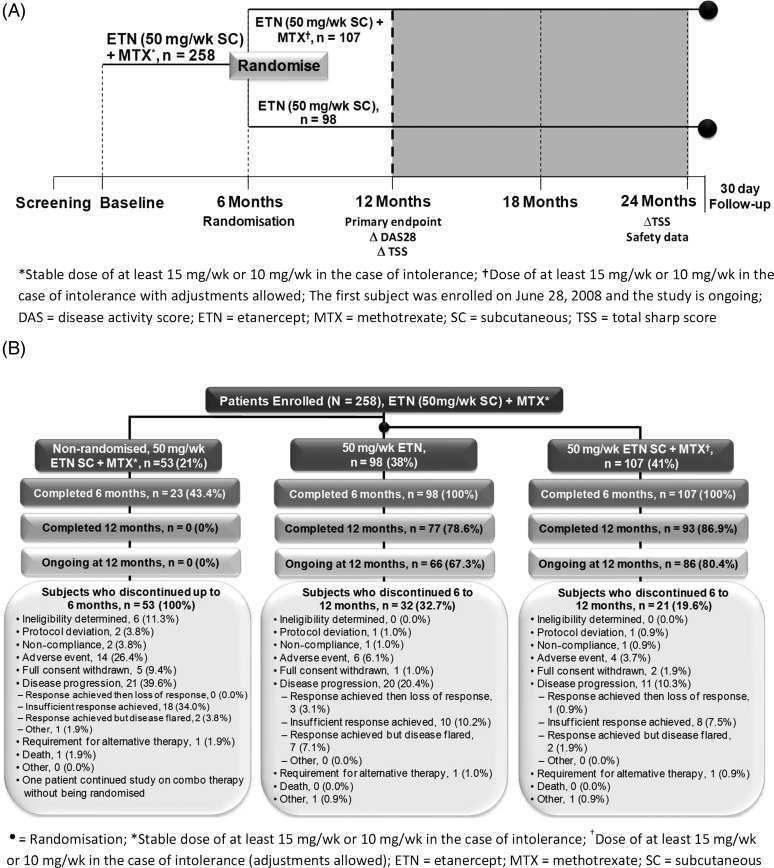
Tumour necrosis factor-inhibitor naïve RA patients with disease activity score 28 (DAS28)≥3.2, swollen joint count≥3, despite stable MTX, were treated with ETN+MTX for 6 months, followed by randomisation to either continue ETN+MTX or switch to ETN monotherapy for an additional 18 months. The primary endpoint was change in DAS28 from 6-month randomisation to 12 months. The non-inferiority margin of change in DAS28 was 0.6, with prespecified analyses (DAS28<3.2 vs DAS28≥3.2).
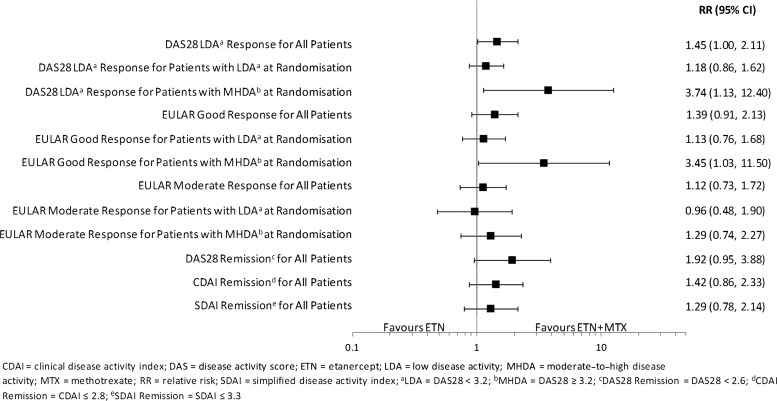
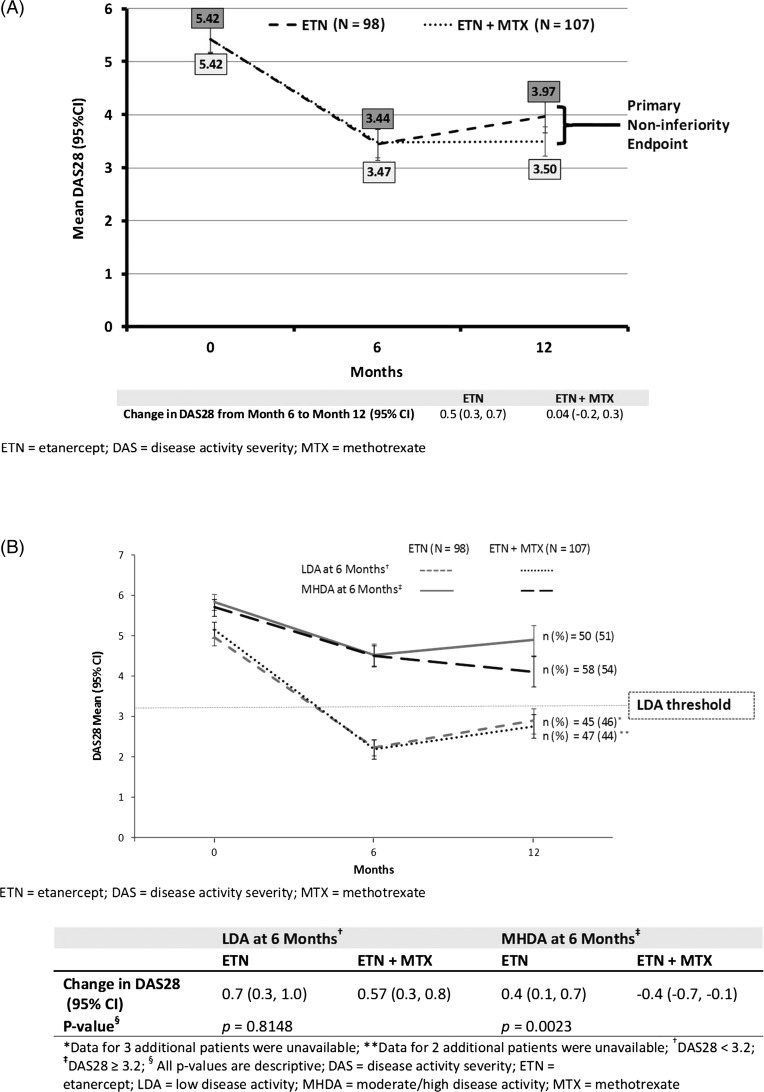
205 patients were randomised. DAS28 was stable in patients on ETN+MTX and increased slightly in patients on ETN monotherapy from 6 to 12 months. Non-inferiority was not achieved, with an adjusted difference of 0.4 (0.1 to 0.7) between the ETN and the ETN+MTX groups, for the month 6-12 change in DAS28. However, patients who achieved low disease activity (LDA; DAS28<3.2) at 6 months had a similar disease activity at 12 months, whether on monotherapy or combination therapy (DAS28 change 0.7 ETN vs 0.57 ETN+MTX, p=0.8148). Conversely, for patients who did not reach LDA at 6 months, those on ETN monotherapy had increased disease activity at 12 months, while disease activity continued to decrease for patients on combination therapy, at 12 months (DAS28 change 0.4 ETN vs -0.4 ETN+MTX, p=0.0023).
Non-inferiority was not achieved. Withdrawing MTX after 6 months of continuation ETN+MTX in MTX inadequate responders did not yield the same degree of improvement between 6 and 12 months compared with continuing ETN+MTX.
ClinicalTrials.gov-NCT00654368.
确定在使用依那西普(ETN)+甲氨蝶呤(MTX)联合治疗6个月后,对于甲氨蝶呤疗效不佳的活动性类风湿关节炎(RA)患者停用MTX是否不劣于继续使用ETN+MTX。
尽管MTX剂量稳定,但疾病活动度评分28(DAS28)≥3.2且肿胀关节计数≥3的未使用过肿瘤坏死因子抑制剂的RA患者,接受ETN+MTX治疗6个月,随后随机分组,分别继续使用ETN+MTX或改用ETN单药治疗18个月。主要终点是从随机分组6个月到12个月时DAS28的变化。DAS28变化的非劣效性界值为0.6,并进行预先设定的分析(DAS28<3.2与DAS28≥3.2)。
205例患者被随机分组。从6个月到12个月,ETN+MTX组患者的DAS28保持稳定,而ETN单药治疗组患者的DAS28略有升高。未达到非劣效性,ETN组与ETN+MTX组在6至12个月DAS28变化方面的调整差异为0.4(0.1至0.7)。然而,在6个月时达到低疾病活动度(LDA;DAS28<3.2)的患者,无论接受单药治疗还是联合治疗,在12个月时疾病活动度相似(DAS28变化:ETN组为0.7,ETN+MTX组为0.57,p = 0.8148)。相反,对于在6个月时未达到LDA的患者,ETN单药治疗组患者在12个月时疾病活动度增加,而联合治疗组患者在12个月时疾病活动度继续下降(DAS28变化:ETN组为0.4,ETN+MTX组为-0.4,p = 0.0023)。
未达到非劣效性。在甲氨蝶呤疗效不佳的患者中,继续使用ETN+MTX 6个月后停用MTX,与继续使用ETN+MTX相比,在6至12个月期间未产生相同程度的改善。
ClinicalTrials.gov - NCT00654368