Dana Center for Preventive Ophthalmology, Johns Hopkins University, Baltimore, Maryland, USA.
PLoS Negl Trop Dis. 2013 Aug 29;7(8):e2415. doi: 10.1371/journal.pntd.0002415. eCollection 2013.
The World Health Organization recommends at least 3 annual antibiotic mass drug administrations (MDA) where the prevalence of trachoma is > 10% in children ages 1-9 years, with coverage at least at 80%. However, the additional value of higher coverage targeted at children with multiple rounds is unknown.
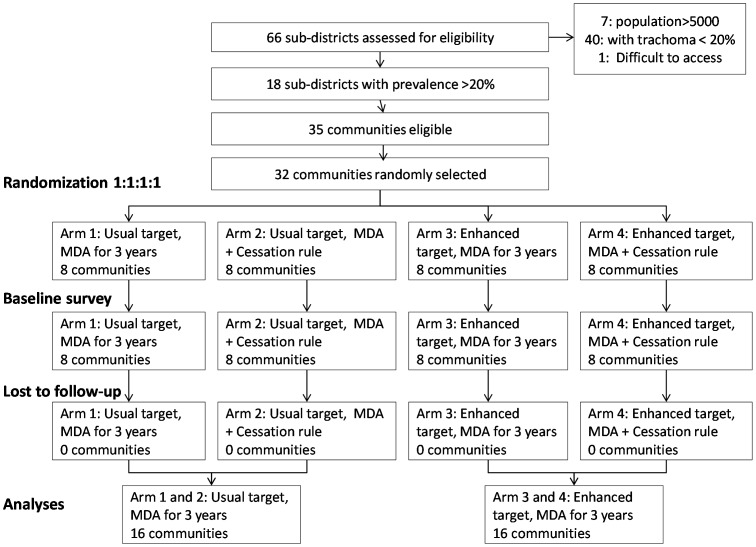
2 × 2 factorial community randomized, double blind, trial.
32 communities with prevalence of trachoma ≥ 20% were randomized to: annual MDA aiming for coverage of children between 80%-90% (usual target) versus aiming for coverag e> 90% (enhanced target); and to: MDA for three years versus a rule of cessation of MDA early if the estimated prevalence of ocular C. trachomatis infection was less than 5%. The primary outcome was the community prevalence of infection with C. trachomatis at 36 months.
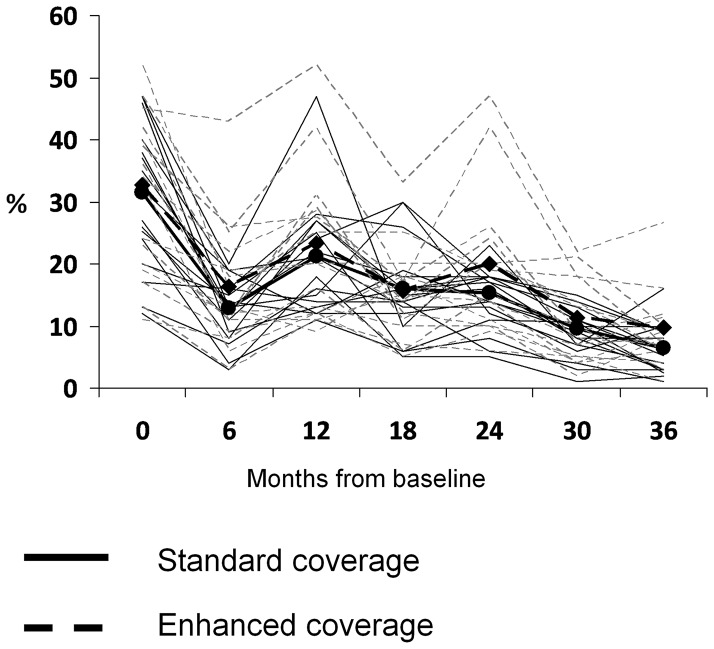
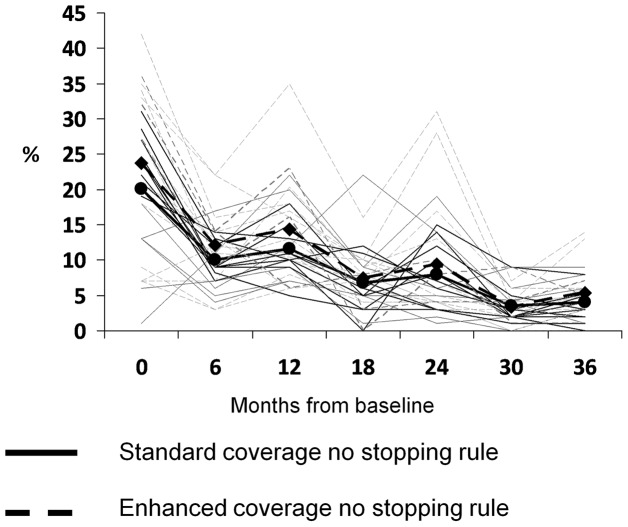
Over the trial's course, no community met the MDA cessation rule, so all communities had the full 3 rounds of MDA. At 36 months, there was no significant difference in the prevalence of infection, 4.0 versus 5.4 (mean adjusted difference = 1.4%, 95% CI = -1.0% to 3.8%), nor in the prevalence of trachoma, 6.1 versus 9.0 (mean adjusted difference = 2.6%, 95% CI = -0.3% to 5.3%) comparing the usual target to the enhanced target group. There was no difference if analyzed using coverage as a continuous variable.
In communities that had pre-treatment prevalence of follicular trachoma of 20% or greater, there is no evidence that MDA can be stopped before 3 annual rounds, even with high coverage. Increasing coverage in children above 90% does not appear to confer additional benefit.
世界卫生组织建议,在儿童中沙眼患病率超过 10%(年龄在 1-9 岁)的地区,每年至少进行 3 次抗生素大规模药物治疗(MDA),覆盖率至少达到 80%。然而,针对多次 MDA 的更高覆盖率的额外价值尚不清楚。
2×2 析因社区随机、双盲试验。
将 32 个沙眼患病率≥20%的社区随机分为两组:每年进行 MDA,目标覆盖率为 80%-90%(常规目标)与目标覆盖率>90%(强化目标);以及 MDA 持续 3 年,或如果估计的眼部沙眼衣原体感染率低于 5%,则提前停止 MDA。主要结局是 36 个月时社区沙眼衣原体感染的患病率。
在试验过程中,没有一个社区符合 MDA 停止规则,因此所有社区都进行了完整的 3 轮 MDA。在 36 个月时,感染率没有显著差异,分别为 4.0%和 5.4%(平均调整差异为 1.4%,95%CI 为-1.0%至 3.8%),也没有差异沙眼患病率,分别为 6.1%和 9.0%(平均调整差异为 2.6%,95%CI 为-0.3%至 5.3%)比较常规目标与强化目标组。使用覆盖率作为连续变量进行分析时,结果也没有差异。
在沙眼滤泡患病率为 20%或更高的社区中,即使覆盖率很高,也没有证据表明 MDA 可以在 3 次年度轮次之前停止。将覆盖率提高到 90%以上的儿童似乎不会带来额外的益处。