Department of Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH; Cleveland Clinic Lerner College of Medicine, Case Western Reserve University, Cleveland, OH; Center for Health Disparities, MetroHealth Medical Center and Case Western Reserve University, Cleveland, OH.
Am J Transplant. 2013 Sep;13(9):2374-83. doi: 10.1111/ajt.12349. Epub 2013 Aug 22.
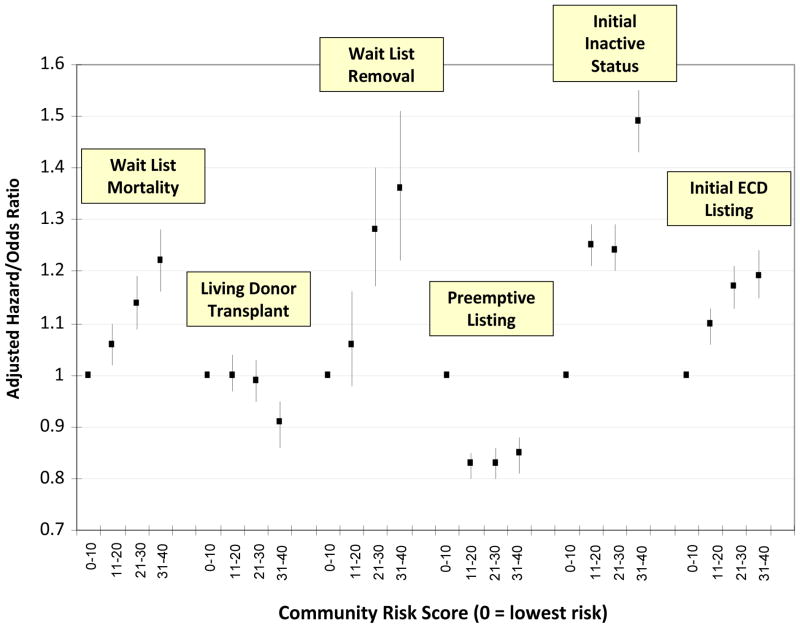
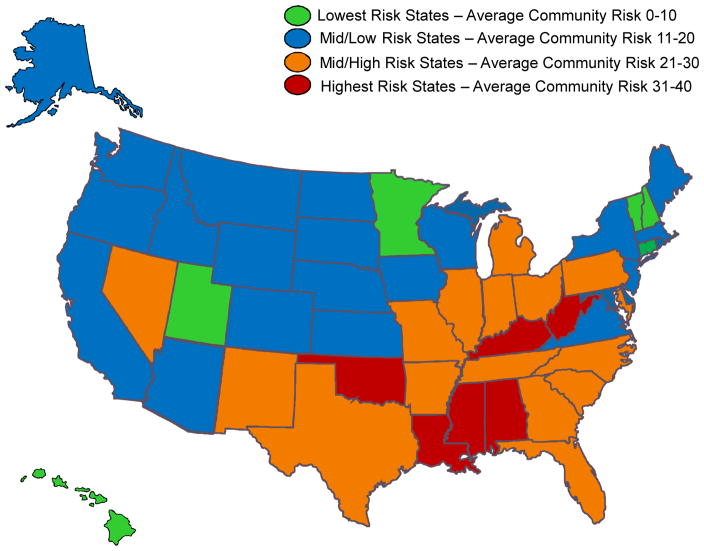
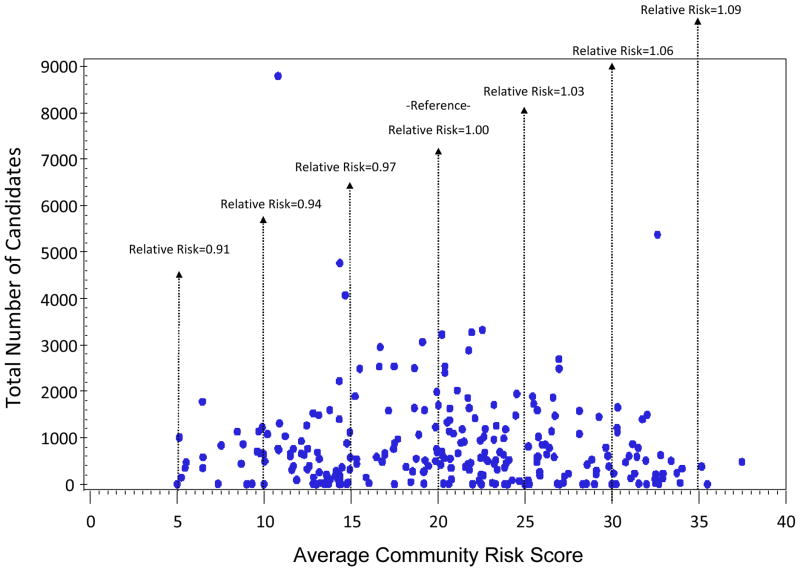
Numerous factors impact patients' health beyond traditional clinical characteristics. We evaluated the association of risk factors in kidney transplant patients' communities with outcomes prior to transplantation. The primary exposure variable was a community risk score (range 0-40) derived from multiple databases and defined by factors including prevalence of comorbidities, access and quality of healthcare, self-reported physical and mental health and socioeconomic status for each U.S. county. We merged data with the Scientific Registry of Transplant Recipients (SRTR) and utilized risk-adjusted models to evaluate effects of community risk for adult candidates listed 2004-2010 (n = 209 198). Patients in highest risk communities were associated with increased mortality (adjusted hazard ratio [AHR] = 1.22, 1.16-1.28), decreased likelihood of living donor transplantation (adjusted odds ratio [AOR] = 0.90, 0.85-0.94), increased waitlist removal for health deterioration (AHR = 1.36, 1.22-1.51), decreased likelihood of preemptive listing (AOR = 0.85, 0.81-0.88), increased likelihood of inactive listing (AOR = 1.49, 1.43-1.55) and increased likelihood of listing for expanded criteria donor kidneys (AHR = 1.19, 1.15-1.24). Associations persisted with adjustment for rural-urban location; furthermore the independent effects of rural-urban location were largely eliminated with adjustment for community risk. Average community risk varied widely by region and transplant center (median = 21, range 5-37). Community risks are powerful factors associated with processes of care and outcomes for transplant candidates and may be important considerations for developing effective interventions and measuring quality of care of transplant centers.
许多因素会影响患者的健康,超出传统的临床特征。我们评估了肾脏移植患者社区中的危险因素与移植前结局的关系。主要暴露变量是一个社区风险评分(范围 0-40),由多个数据库得出,其定义因素包括共病的患病率、医疗保健的可及性和质量、每个美国县的自我报告身心健康和社会经济状况。我们将数据与移植受者科学登记处(SRTR)合并,并利用风险调整模型评估 2004-2010 年列出的成年候选者的社区风险的影响(n = 209198)。处于高风险社区的患者与死亡率增加相关(调整后的危害比 [AHR] = 1.22,1.16-1.28)、活体供者移植的可能性降低(调整后的优势比 [AOR] = 0.90,0.85-0.94)、因健康恶化而从候补名单中删除的可能性增加(AHR = 1.36,1.22-1.51)、抢先列入名单的可能性降低(AOR = 0.85,0.81-0.88)、不活跃列入名单的可能性增加(AOR = 1.49,1.43-1.55)和列入扩展标准供肾的可能性增加(AHR = 1.19,1.15-1.24)。调整城乡位置后,关联仍然存在;此外,通过调整社区风险,城乡位置的独立影响在很大程度上被消除。各地区和移植中心的平均社区风险差异很大(中位数 = 21,范围 5-37)。社区风险是与移植候选者护理过程和结局相关的强大因素,可能是制定有效干预措施和衡量移植中心护理质量的重要考虑因素。