Public Health Sciences, Centre for Population Health Studies, University of Edinburgh,Edinburgh, UK.
BMJ Open. 2013 Sep 13;3(9):e003415. doi: 10.1136/bmjopen-2013-003415.
Inequalities in coronary heart disease mortality by country of birth are large and poorly understood. However, these data misclassify UK-born minority ethnic groups and provide little detail on whether excess risk is due to increased incidence, poorer survival or both.
Retrospective cohort study.
General resident population of Scotland.
All those residing in Scotland during the 2001 Census were eligible for inclusion: 2 972 120 people were included in the analysis. The number still residing in Scotland at the end of the study in 2008 is not known.
As specified in the analysis plan, the primary outcome measures were first occurrence of admission or death due to myocardial infarction and time to event. There were no secondary outcome measures.
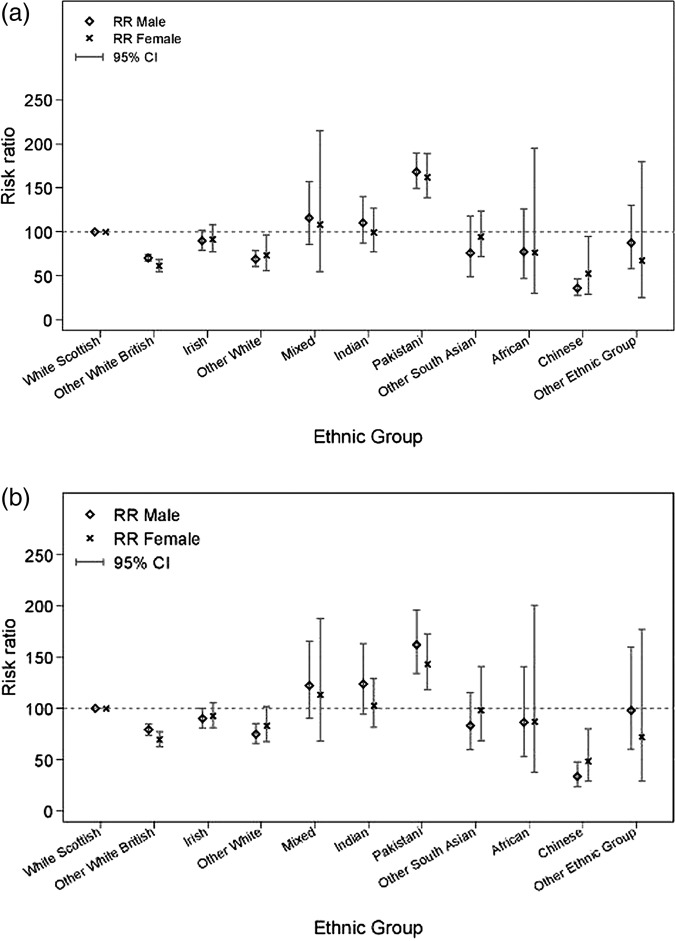
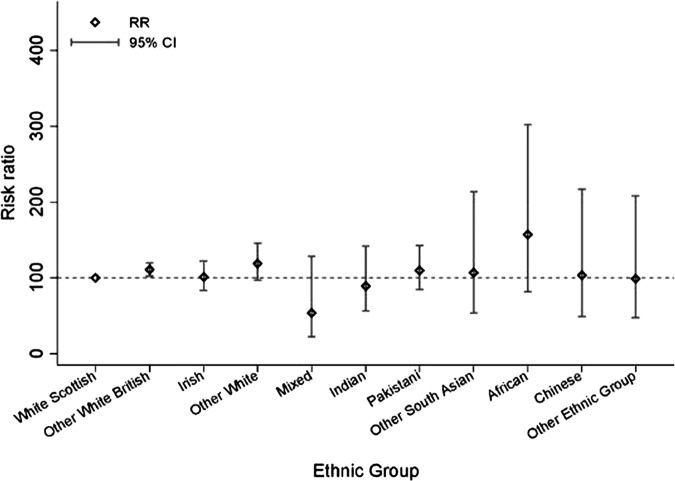
Acute myocardial infarction (AMI) incidence risk ratios (95% CIs) relative to white Scottish populations (100) were highest among Pakistani men (164.1 (142.2 to 189.2)) and women (153.7 (120.5, 196.1)) and lowest for men and women of Chinese (39.5 (27.1 to 57.6) and 59.1 (38.6 to 90.7)), other white British (77 (74.2 to 79.8) and 72.2 (69.0 to 75.5)) and other white (83.1 (75.9 to 91.0) and 79.9 (71.5 to 89.3)) ethnic groups. Adjustment for educational qualification did not eliminate these differences. Cardiac intervention uptake was similar across most ethnic groups. Compared to white Scottish, 28-day survival did not differ by ethnicity, except in Pakistanis where it was better, particularly in women (0.44 (0.25 to 0.78)), a difference not removed by adjustment for education, travel time to hospital or cardiac intervention uptake.
Pakistanis have the highest incidence of AMI in Scotland, a country renowned for internationally high cardiovascular disease rates. In contrast, survival is similar or better in minority ethnic groups. Clinical care and policy should focus on reducing incidence among Pakistanis through more aggressive prevention.
不同出生国的冠心病死亡率存在很大差异,且这一现象的成因尚未被充分理解。然而,这些数据错误地将英国出生的少数族裔归类,并很少详细说明这种超额风险是由于发病率增加、生存率降低还是两者兼而有之。
回顾性队列研究。
苏格兰的一般居民人群。
符合以下条件的所有居民都有资格参与研究:2001 年人口普查时居住在苏格兰的人都被纳入分析;分析共纳入了 2972120 人。截至 2008 年研究结束时,仍居住在苏格兰的人数尚不清楚。
根据分析计划,主要结果测量是首次因心肌梗死住院或死亡的发生和时间。没有次要结果测量。
与苏格兰白人(100)相比,巴基斯坦男性(164.1(142.2 至 189.2))和女性(153.7(120.5 至 196.1))的急性心肌梗死(AMI)发病率风险比(95%CI)最高,而中国男性(39.5(27.1 至 57.6)和女性(59.1(38.6 至 90.7))和其他白种英国人(77(74.2 至 79.8)和 72.2(69.0 至 75.5))和其他白人(83.1(75.9 至 91.0)和 79.9(71.5 至 89.3))的风险比最低。调整教育程度并不能消除这些差异。大多数族裔群体的心脏介入治疗率相似。与苏格兰白人相比,除巴基斯坦人外,28 天生存率因种族而异,而巴基斯坦人,尤其是女性,生存率更好(0.44(0.25 至 0.78)),这种差异在调整教育程度、到医院的旅行时间或心脏介入治疗率后仍然存在。
在苏格兰这个以国际心血管疾病发病率高而闻名的国家,巴基斯坦人患 AMI 的发病率最高。相比之下,少数族裔群体的生存率相似或更高。临床护理和政策应重点通过更积极的预防措施降低巴基斯坦人的发病率。