Applied Kinesiology Laboratory, Program in Physical Therapy, Washington University School of Medicine, St, Louis, MO 63108, USA.
J Foot Ankle Res. 2013 Sep 17;6(1):38. doi: 10.1186/1757-1146-6-38.
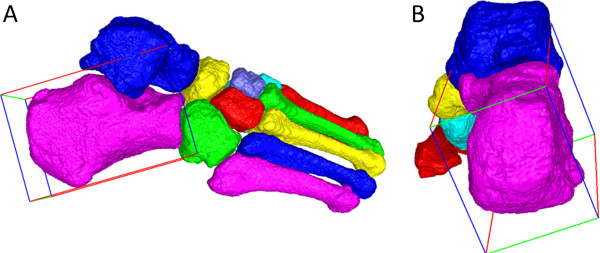
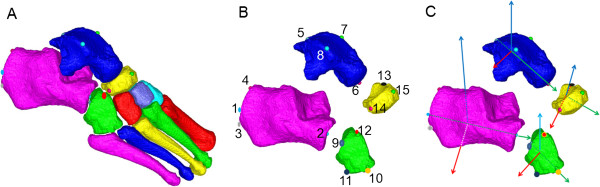
Surgical treatment and clinical management of foot pathology requires accurate, reliable assessment of foot deformities. Foot and ankle deformities are multi-planar and therefore difficult to quantify by standard radiographs. Three-dimensional (3D) imaging modalities have been used to define bone orientations using inertial axes based on bone shape, but these inertial axes can fail to mimic established bone angles used in orthopaedics and clinical biomechanics. To provide improved clinical relevance of 3D bone angles, we developed techniques to define bone axes using landmarks on quantitative computed tomography (QCT) bone surface meshes. We aimed to assess measurement precision of landmark-based, 3D bone-to-bone orientations of hind foot and lesser tarsal bones for expert raters and a template-based automated method.
Two raters completed two repetitions each for twenty feet (10 right, 10 left), placing anatomic landmarks on the surfaces of calcaneus, talus, cuboid, and navicular. Landmarks were also recorded using the automated, template-based method. For each method, 3D bone axes were computed from landmark positions, and Cardan sequences produced sagittal, frontal, and transverse plane angles of bone-to-bone orientations. Angular reliability was assessed using intraclass correlation coefficients (ICCs) and the root mean square standard deviation (RMS-SD) for intra-rater and inter-rater precision, and rater versus automated agreement.
Intra- and inter-rater ICCs were generally high (≥ 0.80), and the ICCs for each rater compared to the automated method were similarly high. RMS-SD intra-rater precision ranged from 1.4 to 3.6° and 2.4 to 6.1°, respectively, for the two raters, which compares favorably to uni-planar radiographic precision. Greatest variability was in Navicular: Talus sagittal plane angle and Cuboid: Calcaneus frontal plane angle. Precision of the automated, atlas-based template method versus the raters was comparable to each rater's internal precision.
Intra- and inter-rater precision suggest that the landmark-based methods have adequate test-retest reliability for 3D assessment of foot deformities. Agreement of the automated, atlas-based method with the expert raters suggests that the automated method is a valid, time-saving technique for foot deformity assessment. These methods have the potential to improve diagnosis of foot and ankle pathologies by allowing multi-planar quantification of deformities.
足部病理学的手术治疗和临床管理需要准确、可靠地评估足部畸形。足部和踝关节畸形是多平面的,因此很难通过标准 X 光片进行量化。三维(3D)成像方式已被用于使用基于骨骼形状的惯性轴来定义骨骼方向,但这些惯性轴可能无法模拟矫形和临床生物力学中使用的既定骨骼角度。为了提高 3D 骨骼角度的临床相关性,我们开发了使用定量计算机断层扫描(QCT)骨骼表面网格上的解剖标志定义骨骼轴的技术。我们的目的是评估专家评估者和基于模板的自动方法对后足和小跗骨的基于标志的 3D 骨骼到骨骼方向的测量精度。
两名评估者分别对二十只脚(10 只右脚,10 只左脚)重复两次,在跟骨、距骨、骰骨和舟骨的表面放置解剖标志。也使用基于模板的自动方法记录了这些标志。对于每种方法,从标志位置计算 3D 骨骼轴,并生成骨骼到骨骼方向矢状面、额状面和横断面角度的卡丹序列。使用组内相关系数(ICC)和内部观察者和外部观察者之间的均方根标准偏差(RMS-SD)评估角度可靠性,以及评估者与自动方法之间的一致性。
内部和外部观察者的 ICC 通常较高(≥0.80),并且每个评估者与自动方法的 ICC 也相似。内部观察者的 RMS-SD 精度范围分别为 1.4 到 3.6°和 2.4 到 6.1°,对于两名评估者来说,这与单平面 X 光片的精度相当。最大的变异性是舟骨:距骨矢状面角度和骰骨:跟骨额状面角度。自动、基于图谱的模板方法与评估者之间的精度与每个评估者的内部精度相当。
内部和外部观察者的精度表明,基于标志的方法对于足部畸形的 3D 评估具有足够的重测可靠性。自动、基于图谱的方法与专家评估者的一致性表明,该自动方法是一种有效的、节省时间的足部畸形评估技术。这些方法有可能通过对畸形进行多平面量化来改善足部和踝关节疾病的诊断。