Xi Jiahe, Shi Wenzhe, Rueckert Daniel, Razavi Reza, Smith Nicolas P, Lamata Pablo
Department of Computer Science, Oxford University, Oxford, UK,
Biomech Model Mechanobiol. 2014 Aug;13(4):747-57. doi: 10.1007/s10237-013-0531-y. Epub 2013 Oct 4.
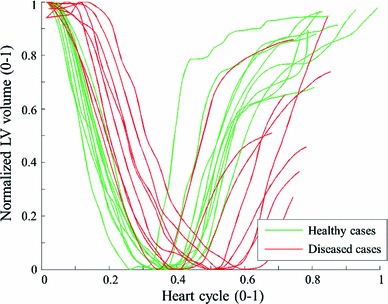
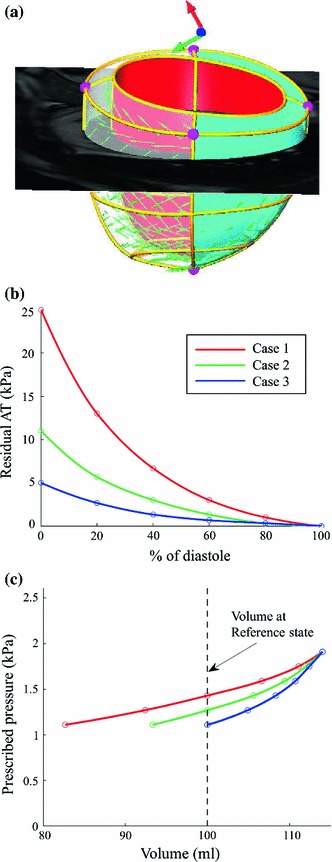
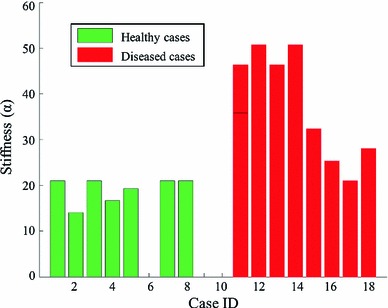
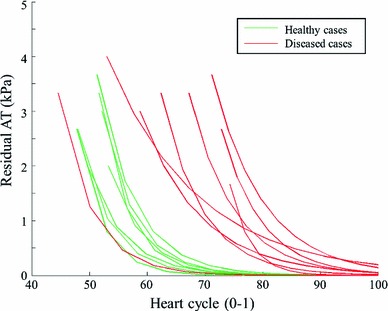
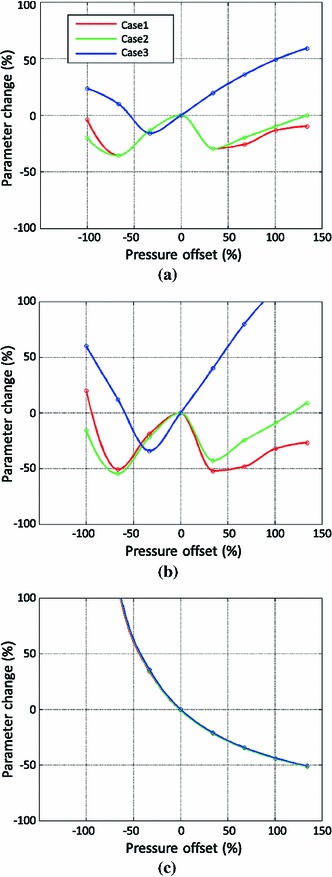
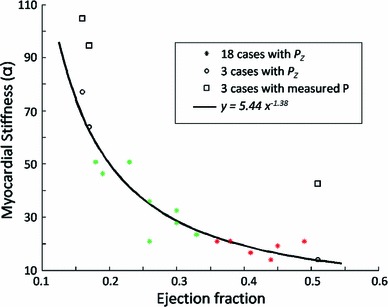
The diastolic function (i.e., blood filling) of the left ventricle (LV) is determined by its capacity for relaxation, or the decay in residual active tension (AT) generated during systole, and its constitutive material properties, or myocardial stiffness. The clinical determination of these two factors (diastolic residual AT and stiffness) is thus essential for assessing LV diastolic function. To quantify these two factors, in our previous work, a novel model-based parameter estimation approach was proposed and successfully applied to multiple cases using clinically acquired motion and invasively measured ventricular pressure data. However, the need to invasively acquire LV pressure limits the wide application of this approach. In this study, we address this issue by analyzing the feasibility of using two kinds of non-invasively available pressure measurements for the purpose of inverse mechanical parameter estimation. The prescription of pressure based on a generic pressure-volume (P-V) relationship reported in literature is first evaluated in a set of 18 clinical cases (10 healthy and 8 diseased), finding reasonable results for stiffness but not for residual active tension. We then investigate the use of non-invasive pressure measures, now available through imaging techniques and limited by unknown or biased offset values. Specifically, three sets of physiologically realistic synthetic data with three levels of diastolic residual active tension (i.e., impaired relaxation capability) are designed to quantify the percentage error in the parameter estimation against the possible pressure offsets within the physiological limits. Maximum errors are quantified as 11 % for the magnitude of stiffness and 22 % for AT, with averaged 0.17 kPa error in pressure measurement offset using the state-of-the-art non-invasive pressure estimation method. The main cause for these errors is the limited temporal resolution of clinical imaging data currently available. These results demonstrate the potential feasibility of the estimation diastolic biomarkers with non-invasive assessment of pressure through medical imaging data.
左心室(LV)的舒张功能(即血液充盈)取决于其舒张能力,或收缩期产生的残余主动张力(AT)的衰减,以及其组成材料特性,即心肌僵硬度。因此,临床确定这两个因素(舒张期残余AT和僵硬度)对于评估左心室舒张功能至关重要。为了量化这两个因素,在我们之前的工作中,提出了一种基于模型的新型参数估计方法,并使用临床获取的运动和侵入性测量的心室压力数据成功应用于多个病例。然而,侵入性获取左心室压力的需求限制了该方法的广泛应用。在本研究中,我们通过分析使用两种非侵入性可用压力测量进行逆向力学参数估计的可行性来解决这个问题。首先在一组18例临床病例(10例健康和8例患病)中评估基于文献报道的通用压力-容积(P-V)关系的压力规定,发现其对僵硬度的结果合理,但对残余主动张力的结果不合理。然后,我们研究使用现在可通过成像技术获得但受未知或有偏差的偏移值限制的非侵入性压力测量。具体而言,设计了三组具有三种舒张期残余主动张力水平(即舒张能力受损)的生理现实合成数据,以量化针对生理极限内可能的压力偏移的参数估计中的百分比误差。使用最先进的非侵入性压力估计方法,僵硬度大小的最大误差量化为11%,AT的最大误差量化为22%,压力测量偏移的平均误差为0.17 kPa。这些误差的主要原因是当前可用临床成像数据的时间分辨率有限。这些结果证明了通过医学成像数据进行压力的非侵入性评估来估计舒张期生物标志物的潜在可行性。