Department of Epidemiology, Mailman School of Public Health, Columbia University, New York, NY.
J Am Heart Assoc. 2013 Oct 28;2(6):e000254. doi: 10.1161/JAHA.113.000254.
No prospective studies exist on the relationship between change in periodontal clinical and microbiological status and progression of carotid atherosclerosis.
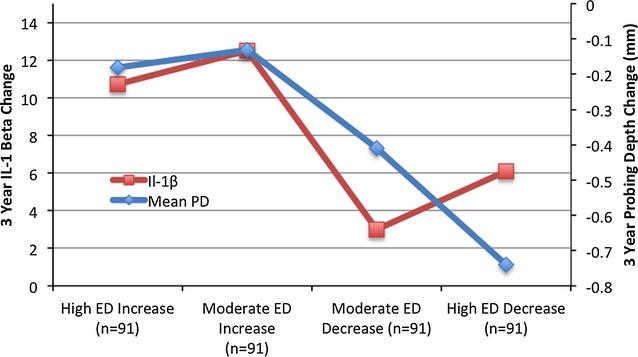
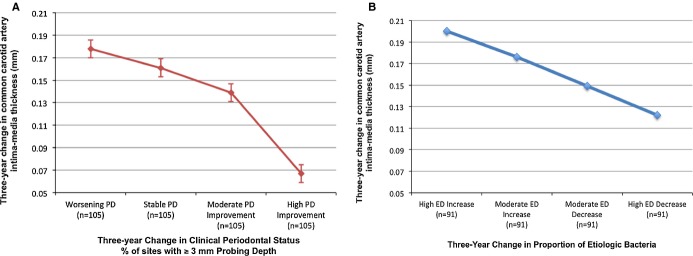
The Oral Infections and Vascular Disease Epidemiology Study examined 420 participants at baseline (68 ± 8 years old) and follow-up. Over a 3-year median follow-up time, clinical probing depth (PD) measurements were made at 75 766 periodontal sites, and 5008 subgingival samples were collected from dentate participants (average of 7 samples/subject per visit over 2 visits) and quantitatively assessed for 11 known periodontal bacterial species by DNA-DNA checkerboard hybridization. Common carotid artery intima-medial thickness (CCA-IMT) was measured using high-resolution ultrasound. In 2 separate analyses, change in periodontal status (follow-up to baseline), defined as (1) longitudinal change in the extent of sites with a ≥ 3-mm probing depth (Δ%PD ≥ 3) and (2) longitudinal change in the relative predominance of bacteria causative of periodontal disease over other bacteria in the subgingival plaque (Δetiologic dominance), was regressed on longitudinal CCA-IMT progression adjusting for age, sex, race/ethnicity, diabetes, smoking status, education, body mass index, systolic blood pressure, and low-density lipoprotein cholesterol and high-density lipoprotein cholesterol. Mean (SE) CCA-IMT increased during follow-up by 0.139 ± 0.008 mm. Longitudinal IMT progression attenuated with improvement in clinical or microbial periodontal status. Mean CCA-IMT progression varied inversely across quartiles of longitudinal improvement in clinical periodontal status (Δ%PD ≥ 3) by 0.18 (0.02), 0.16 (0.01), 0.14 (0.01), and 0.07 (0.01) mm (P for trend<0.0001). Likewise, mean CCA-IMT increased by 0.20 (0.02), 0.18 (0.02), 0.15 (0.02), and 0.12 (0.02) mm (P<0.0001) across quartiles of longitudinal improvement in periodontal microbial status (Δetiologic dominance).
Longitudinal improvement in clinical and microbial periodontal status is related to a decreased rate of carotid artery IMT progression at 3-year average follow-up.
目前尚无前瞻性研究探讨牙周临床和微生物状况的变化与颈动脉粥样硬化进展之间的关系。
口腔感染和血管疾病流行病学研究在基线(68±8 岁)和随访时检查了 420 名参与者。在中位随访时间 3 年期间,对 75766 个牙周部位进行了临床探诊深度(PD)测量,并从有牙参与者中采集了 5008 个龈下样本(每次就诊平均采集 7 个样本/受试者,共采集 2 次就诊),并通过 DNA-DNA 斑点杂交定量评估 11 种已知的牙周致病菌。采用高分辨率超声测量颈总动脉内膜-中层厚度(CCA-IMT)。在 2 项单独的分析中,牙周状况的变化(随访至基线),定义为(1)≥3mm 探诊深度的部位比例的纵向变化(Δ%PD≥3)和(2)龈下斑块中导致牙周病的细菌相对于其他细菌的纵向优势变化(Δ病因优势),与调整年龄、性别、种族/民族、糖尿病、吸烟状况、教育程度、体重指数、收缩压、低密度脂蛋白胆固醇和高密度脂蛋白胆固醇后纵向 CCA-IMT 进展进行回归分析。在随访期间,平均(SE)CCA-IMT 增加了 0.139±0.008mm。随着临床或微生物牙周状况的改善,纵向 IMT 进展减弱。CCA-IMT 进展的平均变化在临床牙周状况纵向改善的四分位区间内呈反比变化(Δ%PD≥3),分别为 0.18(0.02)、0.16(0.01)、0.14(0.01)和 0.07(0.01)mm(P<0.0001)。同样,CCA-IMT 也随着牙周微生物状况纵向改善的四分位区间(Δ病因优势)而增加,分别为 0.20(0.02)、0.18(0.02)、0.15(0.02)和 0.12(0.02)mm(P<0.0001)。
在 3 年的平均随访中,临床和微生物牙周状况的纵向改善与颈动脉 IMT 进展速度的降低有关。