Adrie Christophe, Schwebel Carole, Garrouste-Orgeas Maïté, Vignoud Lucile, Planquette Benjamin, Azoulay Elie, Kallel Hatem, Darmon Michael, Souweine Bertrand, Dinh-Xuan Anh-Tuan, Jamali Samir, Zahar Jean-Ralph, Timsit Jean-François
Crit Care. 2013 Nov 7;17(6):R265. doi: 10.1186/cc13095.
Several guidelines recommend initial empirical treatment with two antibiotics instead of one to decrease mortality in community-acquired pneumonia (CAP) requiring intensive-care-unit (ICU) admission. We compared the impact on 60-day mortality of using one or two antibiotics. We also compared the rates of nosocomial pneumonia and multidrug-resistant bacteria.
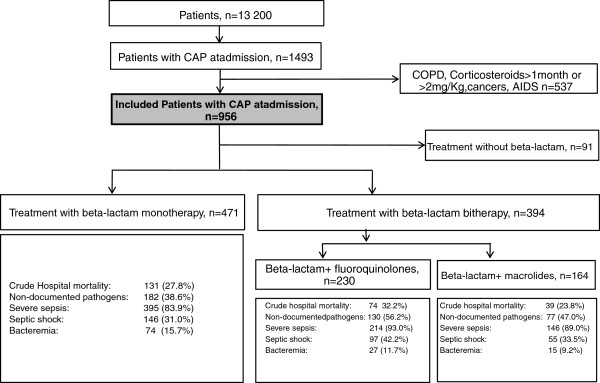
This is an observational cohort study of 956 immunocompetent patients with CAP admitted to ICUs in France and entered into a prospective database between 1997 and 2010.
Initial adequate antibiotic therapy was significantly associated with better survival (subdistribution hazard ratio (sHR), 0.63; 95% confidence interval (95% CI), 0.42 to 0.94; P = 0.02); this effect was strongest in patients with Streptococcus pneumonia CAP (sHR, 0.05; 95% CI, 0.005 to 0.46; p = 0.001) or septic shock (sHR: 0.62; 95% CI 0.38 to 1.00; p = 0.05). Dual therapy was associated with a higher frequency of initial adequate antibiotic therapy. However, no difference in 60-day mortality was found between monotherapy (β-lactam) and either of the two dual-therapy groups (β-lactam plus macrolide or fluoroquinolone). The rates of nosocomial pneumonia and multidrug-resistant bacteria were not significantly different across these three groups.
Initial adequate antibiotic therapy markedly decreased 60-day mortality. Dual therapy improved the likelihood of initial adequate therapy but did not predict decreased 60-day mortality. Dual therapy did not increase the risk of nosocomial pneumonia or multidrug-resistant bacteria.
多项指南推荐,对于需要入住重症监护病房(ICU)的社区获得性肺炎(CAP)患者,初始经验性治疗采用两种抗生素而非一种,以降低死亡率。我们比较了使用一种或两种抗生素对60天死亡率的影响。我们还比较了医院获得性肺炎和多重耐药菌的发生率。
这是一项对956例免疫功能正常的CAP患者进行的观察性队列研究,这些患者于1997年至2010年间入住法国的ICU,并被纳入一个前瞻性数据库。
初始充分的抗生素治疗与更好的生存率显著相关(亚分布风险比[sHR],0.63;95%置信区间[95%CI],0.42至0.94;P = 0.02);这种效应在肺炎链球菌CAP患者(sHR,0.05;95%CI,0.005至0.46;p = 0.001)或感染性休克患者中最为明显(sHR:0.62;95%CI 0.38至1.00;p = 0.05)。联合治疗与初始充分抗生素治疗的更高频率相关。然而,单药治疗(β-内酰胺类)与两个联合治疗组(β-内酰胺类加大环内酯类或氟喹诺酮类)中的任何一组在60天死亡率上均未发现差异。这三组的医院获得性肺炎和多重耐药菌发生率无显著差异。
初始充分的抗生素治疗显著降低了60天死亡率。联合治疗提高了初始充分治疗的可能性,但并未预测60天死亡率的降低。联合治疗并未增加医院获得性肺炎或多重耐药菌的风险。