Pfizer Oncology, 10646 Science Center Drive, La Jolla, San Diego, CA, 92121, USA.
Cancer Chemother Pharmacol. 2014 Jan;73(1):151-61. doi: 10.1007/s00280-013-2333-4. Epub 2013 Nov 13.
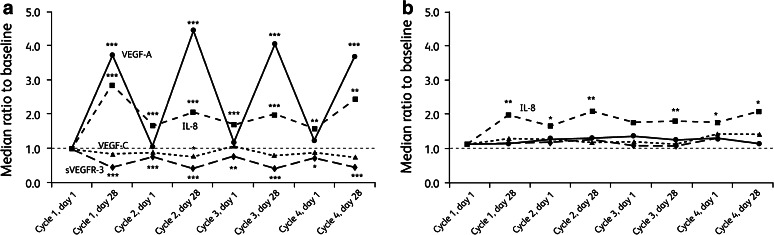
We investigated potential biomarkers of efficacy in a phase III trial of sunitinib versus interferon-alpha (IFN-α), first-line in metastatic renal cell carcinoma (mRCC), by analyzing plasma levels of vascular endothelial growth factor (VEGF)-A, VEGF-C, soluble VEGF receptor-3 (sVEGFR-3) and interleukin (IL)-8.
Seven hundred and fifty mRCC patients were randomized to oral sunitinib 50 mg/day in repeated cycles of a 4-week on/2-week off schedule or IFN-α 9 million units subcutaneously thrice weekly. Plasma samples collected from a subset of 63 patients on days 1 and 28 of cycles 1-4 and at end of treatment were analyzed by ELISA.
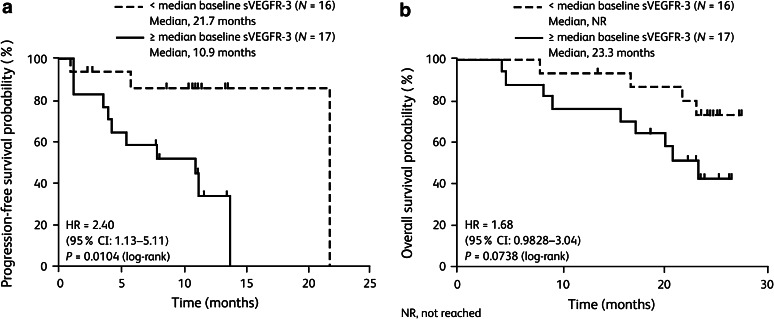
Baseline characteristics of biomarker-evaluated patients in sunitinib (N = 33) and IFN-α (N = 30) arms were comparable to their respective intent-to-treat populations. By univariate Cox regression analysis, low baseline soluble protein levels were associated with lower risk of progression/death (all P < 0.05): in both treatment arms, baseline VEGF-A and IL-8 were associated with overall survival (OS) and baseline VEGF-C with progression-free survival (PFS); in the sunitinib arm, baseline VEGF-A was associated with PFS and baseline sVEGFR-3 with PFS and OS; in the IFN-α arm, baseline IL-8 was associated with PFS. In multivariate analysis, baseline sVEGFR-3 and IL-8 remained independent predictors of OS in the sunitinib arm, while no independent predictors of outcome remained in the IFN-α arm. Pharmacodynamic changes were not associated with PFS or OS for any plasma protein investigated.
Our findings suggest that, in mRCC, baseline VEGF-A and IL-8 may have prognostic value, while baseline sVEGFR-3 may predict sunitinib efficacy.
通过分析血管内皮生长因子(VEGF)-A、VEGF-C、可溶性 VEGF 受体-3(sVEGFR-3)和白细胞介素(IL)-8 的血浆水平,我们研究了舒尼替尼与干扰素-α(IFN-α)一线治疗转移性肾细胞癌(mRCC)的 III 期试验中疗效的潜在生物标志物。
750 名 mRCC 患者被随机分配接受舒尼替尼 50mg/天,每天口服,每 4 周一个周期,其中 2 周停药,或 IFN-α 900 万单位皮下注射,每周 3 次。在第 1 周期和第 4 周期的第 1 天和第 28 天以及治疗结束时,从 63 名患者中采集的血浆样本通过 ELISA 进行分析。
在舒尼替尼(N=33)和 IFN-α(N=30)组中,接受生物标志物评估的患者的基线特征与各自的意向治疗人群相当。通过单变量 Cox 回归分析,低基线可溶性蛋白水平与进展/死亡风险较低相关(均 P <0.05):在两个治疗组中,基线 VEGF-A 和 IL-8 与总生存期(OS)相关,基线 VEGF-C 与无进展生存期(PFS)相关;在舒尼替尼组中,基线 VEGF-A 与 PFS 相关,基线 sVEGFR-3 与 PFS 和 OS 相关;在 IFN-α 组中,基线 IL-8 与 PFS 相关。多变量分析中,基线 sVEGFR-3 和 IL-8 仍然是舒尼替尼组 OS 的独立预测因素,而 IFN-α 组中没有独立的预后预测因素。任何研究的血浆蛋白的药效学变化均与 PFS 或 OS 无关。
我们的研究结果表明,在 mRCC 中,基线 VEGF-A 和 IL-8 可能具有预后价值,而基线 sVEGFR-3 可能预测舒尼替尼的疗效。