Centre for Communicable Diseases and Infection Control, Infectious Disease Prevention and Control Branch, Public Health Agency of Canada, Ottawa, Ontario, Canada.
PLoS One. 2013 Nov 27;8(11):e80481. doi: 10.1371/journal.pone.0080481. eCollection 2013.
Poisson regression modelling has been widely used to estimate the disease burden attributable to influenza, though not without concerns that some of the excess burden could be due to other causes. This study aims to provide annual estimates of the mortality and hospitalization burden attributable to both seasonal influenza and the 2009 A/H1N1 pandemic influenza for Canada, and to discuss issues related to the reliability of these estimates.
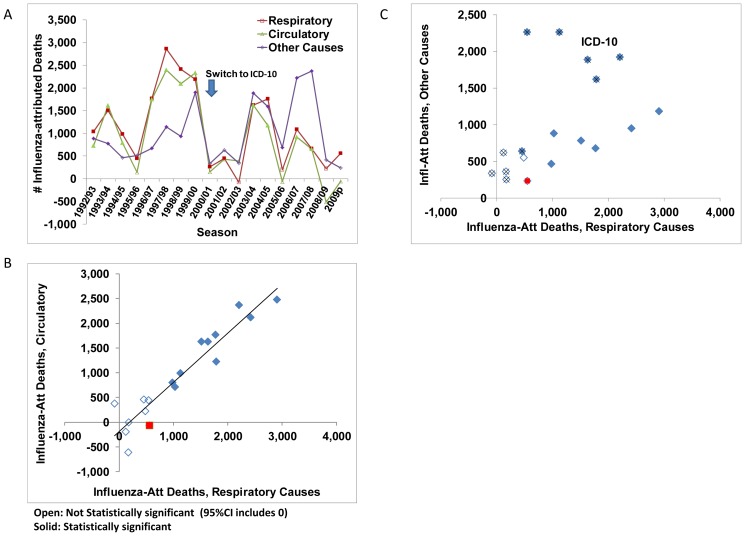
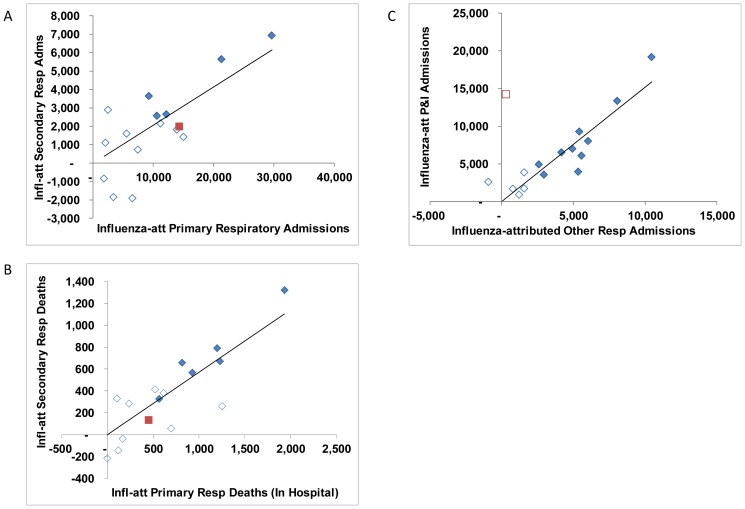
Weekly time-series for all-cause mortality and regression models were used to estimate the number of deaths in Canada attributable to influenza from September 1992 to December 2009. To assess their robustness, the annual estimates derived from different parameterizations of the regression model for all-cause mortality were compared. In addition, the association between the annual estimates for mortality and hospitalization by age group, underlying cause of death or primary reason for admission and discharge status is discussed.
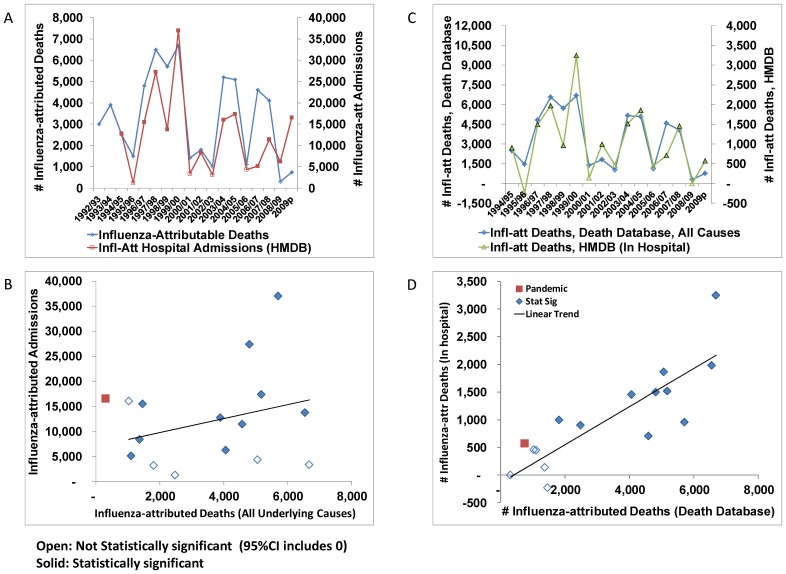
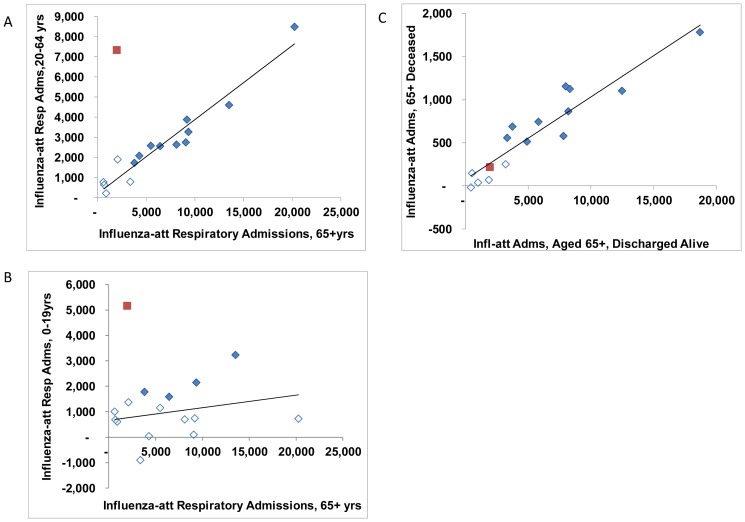
The crude influenza-attributed mortality rate based on all-cause mortality and averaged over 17 influenza seasons prior to the 2009 A/H1N1 pandemic was 11.3 (95%CI, 10.5 - 12.1) deaths per 100 000 population per year, or an average of 3,500 (95%CI, 3,200 - 3,700) deaths per year attributable to seasonal influenza. The estimated annual rates ranged from undetectable at the ecological level to more than 6000 deaths per year over the three A/Sydney seasons. In comparison, we attributed an estimated 740 deaths (95%CI, 350-1500) to A(H1N1)pdm09. Annual estimates from different model parameterizations were strongly correlated, as were estimates for mortality and morbidity; the higher A(H1N1)pdm09 burden in younger age groups was the most notable exception.
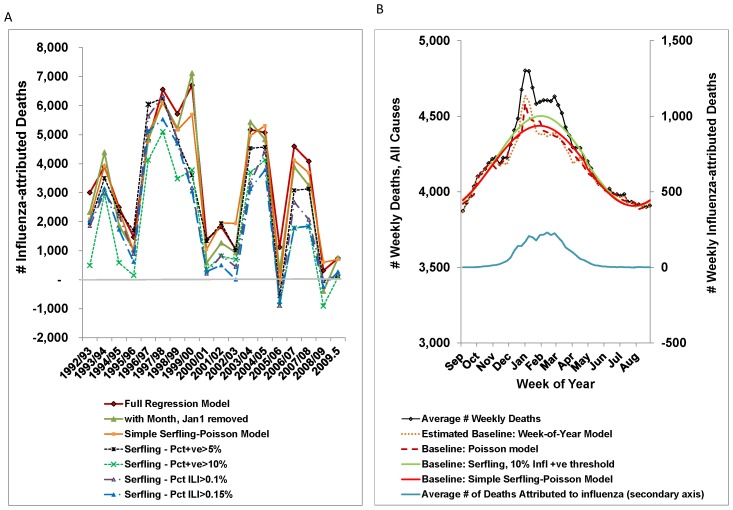
With the exception of some of the Serfling models, differences in the ecological estimates of the disease burden attributable to influenza were small in comparison to the variation in disease burden from one season to another.
泊松回归模型已广泛用于估计流感造成的疾病负担,但也有人担心,其中一些超额负担可能是由其他原因造成的。本研究旨在为加拿大提供季节性流感和 2009 年 A/H1N1 大流行流感造成的死亡率和住院负担的年度估计,并讨论与这些估计的可靠性相关的问题。
使用全因死亡率的每周时间序列和回归模型来估计 1992 年 9 月至 2009 年 12 月期间加拿大流感造成的死亡人数。为了评估其稳健性,比较了全因死亡率回归模型的不同参数化方法得出的年度估计值。此外,还讨论了年龄组、根本死因或入院和出院状况的主要原因之间与死亡率和住院率年度估计值的相关性。
在 2009 年 A/H1N1 大流行之前的 17 个流感季节,基于全因死亡率的粗流感归因死亡率平均为每 10 万人每年 11.3(95%CI,10.5-12.1)例死亡,即每年平均有 3500(95%CI,3200-3700)例死亡归因于季节性流感。估计的年度发病率从生态学水平上无法检测到,到三个 A/Sydney 季节每年超过 6000 例死亡不等。相比之下,我们估计 A(H1N1)pdm09 导致 740 人死亡(95%CI,350-1500)。不同模型参数化的年度估计值高度相关,死亡率和发病率的估计值也高度相关;年龄较小的年龄组中 A(H1N1)pdm09 负担较高是最显著的例外。
除了一些 Serfling 模型外,与流感造成的疾病负担的季节性变化相比,流感造成的疾病负担的生态学估计值差异较小。