Department of Cardiovascular Surgery, Osaka City University Graduate School of Medicine, 1-4-3 Asahi-machi, Abeno-ku, Osaka 545-8585, Japan.
World J Surg Oncol. 2013 Dec 6;11:309. doi: 10.1186/1477-7819-11-309.
Radical segmentectomy has been performed for small-sized non-small cell lung cancer (NSCLC). However, underestimation of mediastinal lymph node metastasis in the absence of hilar or interlobar metastasis (skip N2) affects surgical strategy. Our aim was to investigate preoperative and intraoperative predictors of skip N2 in clinical stage (c-stage) IA NSCLC.
From 1998 to 2011, 279 patients (155 men and 124 women) with c-stage IA NSCLC (230 pN0, 17 pN1, 12 skip N2, 20 non-skip N2) underwent systematic lobectomy (R0 resection) at our institute. We compared preoperative serum concentrations of carcinoembryonic antigen, cytokeratin 19 fragment, sialyl Lewis X (SLX), and pre- and intraoperative clinicopathological features of pN0 and skip N2 patients. Receiver operator characteristic (ROC) curve analysis was performed to distinguish between the two patient groups.
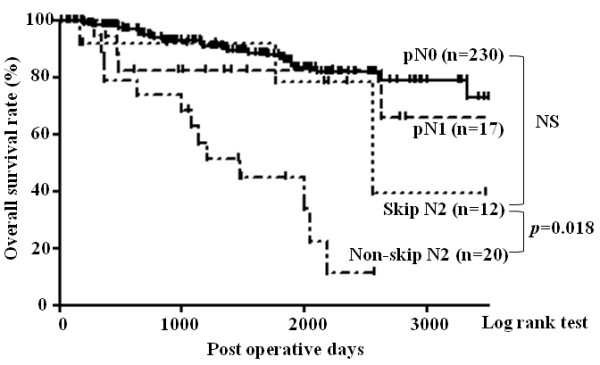
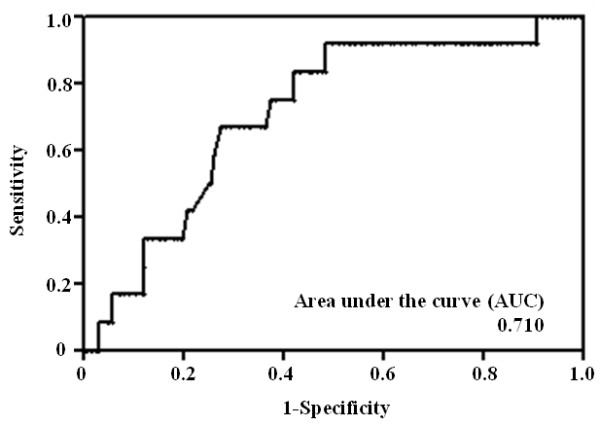
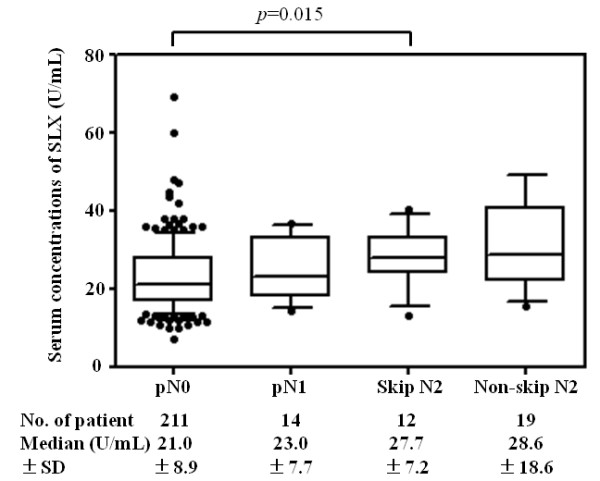
The 5-year survival rate of skip N2 patients was 78.6%, higher than that of non-skip N2 patients (44.9%), and not significantly different than that of pN0 (86.7%) or pN1 patients (82.4%). The mean serum SLX concentration in skip N2 patients (28.0 U/ml) was elevated compared to that in pN0 patients (22.9 U/ml). In ROC analysis of SLX, the area under the curve was 0.710, and the optimal cut-off value was 21.4 U/ml (sensitivity, 91.7%; specificity, 51.7%). In multivariate analysis, SLX was an independent predictor of skip N2 in patients with c-stage IA NSCLC (odds ratio, 9.43; p = 0.006).
Skip N2 metastasis is common in patients with c-stage IA NSCLC with high serum SLX, and lobectomy with complete dissection of hilar and mediastinal lymph nodes should remain the standard surgical procedure for these cases.
对于小尺寸非小细胞肺癌(NSCLC),已施行根治性节段切除术。然而,在无肺门或叶间转移(跳跃性 N2)的情况下,对纵隔淋巴结转移的低估会影响手术策略。我们的目的是探讨临床分期(c 期)IA 期非小细胞肺癌中跳跃性 N2 的术前和术中预测因素。
1998 年至 2011 年,我院对 279 例 c 期 IA 期 NSCLC 患者(230 例 pN0、17 例 pN1、12 例跳跃性 N2、20 例非跳跃性 N2)进行了系统性肺叶切除术(R0 切除)。我们比较了 pN0 和跳跃性 N2 患者的术前血清癌胚抗原、细胞角蛋白 19 片段、唾液酸化路易斯 X(SLX)浓度以及术前和术中临床病理特征。通过接收者操作特征(ROC)曲线分析来区分两组患者。
跳跃性 N2 患者的 5 年生存率为 78.6%,高于非跳跃性 N2 患者(44.9%),但与 pN0 患者(86.7%)或 pN1 患者(82.4%)无显著差异。跳跃性 N2 患者的平均血清 SLX 浓度(28.0 U/ml)高于 pN0 患者(22.9 U/ml)。在 SLX 的 ROC 分析中,曲线下面积为 0.710,最佳截断值为 21.4 U/ml(敏感性,91.7%;特异性,51.7%)。在多变量分析中,SLX 是 c 期 IA 期非小细胞肺癌患者跳跃性 N2 的独立预测因素(优势比,9.43;p=0.006)。
c 期 IA 期非小细胞肺癌患者的跳跃性 N2 转移较为常见,血清 SLX 水平较高,对于这些病例,肺叶切除术联合肺门和纵隔淋巴结完全清扫仍应作为标准手术方法。