Department of Population Health, New York University School of Medicine, New York, NY.
J Am Heart Assoc. 2013 Dec 13;2(6):e000505. doi: 10.1161/JAHA.113.000505.
Exercise testing with echocardiography or myocardial perfusion imaging is widely used to risk-stratify patients with suspected coronary artery disease. However, reports of diagnostic performance rarely adjust for referral bias, and this practice may adversely influence patient care. Therefore, we evaluated the potential impact of referral bias on diagnostic effectiveness and clinical decision-making.
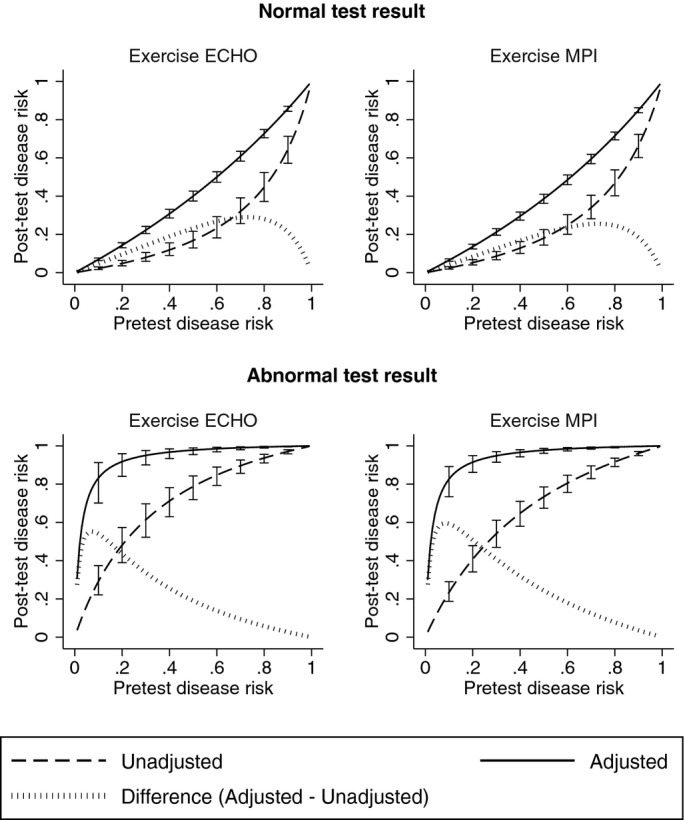
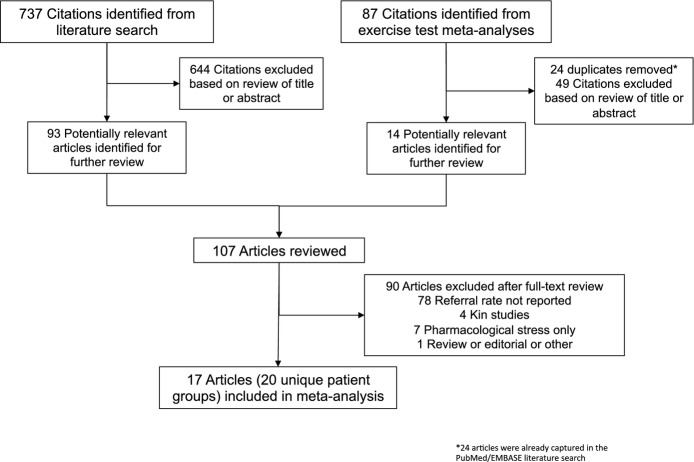
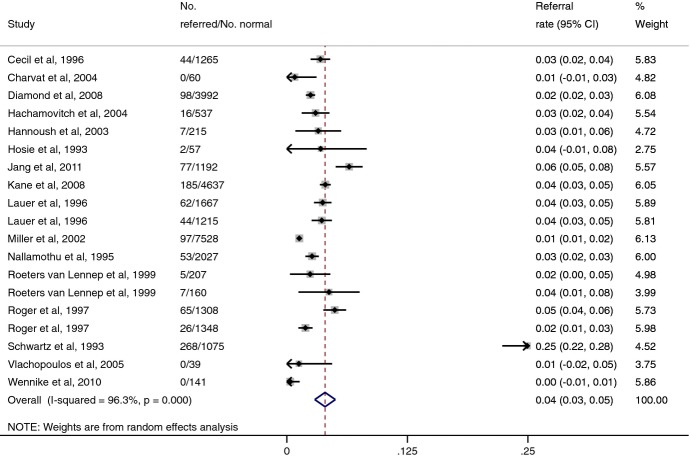
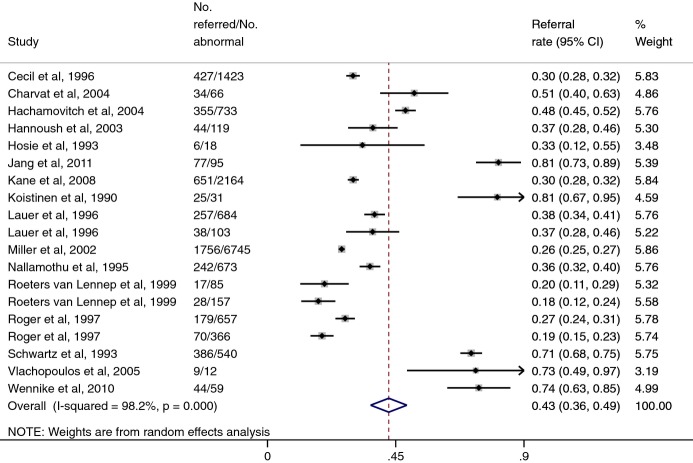
Searching PubMed and EMBASE (1990-2012), 2 investigators independently evaluated eligibility and abstracted data on study characteristics and referral patterns. Diagnostic performance reported in 4 previously published meta-analyses of exercise echocardiography and myocardial perfusion imaging was adjusted using pooled referral rates and Bayesian methods. Twenty-one studies reported referral patterns in 49 006 patients (mean age 60.7 years, 39.6% women, and 0.8% prior history of myocardial infarction). Catheterization referral rates after normal and abnormal exercise tests were 4.0% (95% CI, 2.9% to 5.0%) and 42.5% (36.2% to 48.9%), respectively, with odds ratio for referral after an abnormal test of 14.6 (10.7 to 19.9). After adjustment for referral, exercise echocardiography sensitivity fell from 84% (80% to 89%) to 34% (27% to 41%), and specificity rose from 77% (69% to 86%) to 99% (99% to 100%). Similarly, exercise myocardial perfusion imaging sensitivity fell from 85% (81% to 88%) to 38% (31% to 44%), and specificity rose from 69% (61% to 78%) to 99% (99% to 100%). Summary receiver operating curve analysis demonstrated only modest changes in overall discriminatory power but adjusting for referral increased positive-predictive value and reduced negative-predictive value.
Exercise echocardiography and myocardial perfusion imaging are considerably less sensitive and more specific for coronary artery disease after adjustment for referral. Given these findings, future work should assess the comparative ability of these and other tests to rule-in versus rule-out coronary artery disease.
超声心动图或心肌灌注成像的运动试验广泛用于对疑似冠心病患者进行风险分层。然而,很少有研究报告对诊断性能进行调整,以消除转诊偏倚,而这种做法可能会对患者的治疗产生不利影响。因此,我们评估了转诊偏倚对诊断效能和临床决策的潜在影响。
通过检索 PubMed 和 EMBASE(1990-2012 年),两名研究者独立评估了研究特征和转诊模式的入选标准和摘要数据。使用汇总的转诊率和贝叶斯方法对 4 项先前发表的运动超声心动图和心肌灌注成像荟萃分析中报告的诊断性能进行了调整。21 项研究报告了 49006 例患者(平均年龄 60.7 岁,39.6%为女性,0.8%有心肌梗死既往史)的转诊模式。正常和异常运动试验后的导管插入术转诊率分别为 4.0%(95%CI:2.9%至 5.0%)和 42.5%(36.2%至 48.9%),异常试验后转诊的优势比为 14.6(10.7 至 19.9)。调整转诊后,运动超声心动图的敏感性从 84%(80%至 89%)降至 34%(27%至 41%),特异性从 77%(69%至 86%)升至 99%(99%至 100%)。同样,运动心肌灌注成像的敏感性从 85%(81%至 88%)降至 38%(31%至 44%),特异性从 69%(61%至 78%)升至 99%(99%至 100%)。汇总受试者工作特征曲线分析表明,整体判别能力仅有适度变化,但调整转诊后可提高阳性预测值,降低阴性预测值。
调整转诊后,超声心动图和心肌灌注成像对冠状动脉疾病的敏感性明显降低,特异性明显升高。鉴于这些发现,未来的研究应评估这些和其他检查方法对冠状动脉疾病的排除和确诊能力。