Primary Care Center Jakobsgårdarna, Jaxtorget 7A, Box 100 33 Borlänge S-781 10, Sweden.
BMC Pregnancy Childbirth. 2013 Dec 17;13:237. doi: 10.1186/1471-2393-13-237.
Severe vitamin D deficiency can impair muscle strength. The study aims were to examine physical performance in the hands and upper legs, and analyze plasma 25-hydroxyvitamin D (25(OH)D) concentrations in women with presumably low (veiled, Somali-born) and high levels (unveiled, Swedish-born).
Women (n=123, 58% Swedish) enrolled at a Swedish antenatal clinic, latitude 60° N, were recruited. Plasma 25(OH) D was analyzed, measured as nmol/L, then categorized as <10 = undetectable, 10-24, 25-49, 50-74 or >75. Muscle strength was tested: maximal hand grip strength (in Newtons, N), and upper leg performance (categorized as able/unable to perform squatting, standing on one leg, standing from a chair, and lifting their hips). Social and anthropometric data were collected. Non-parametric statistics tested the data for differences in their ability to perform the tests across 25(OH)D categories. Undetectable values (<10 nmol/L) were replaced with '9' in the linear correlation statistics. A final main effect model for grip strength (in N) was calculated using stepwise linear regression for independent variables: country of birth, 25(OH)D levels, age, height, weight, physical activity, lactation status, parity, and gestational age.
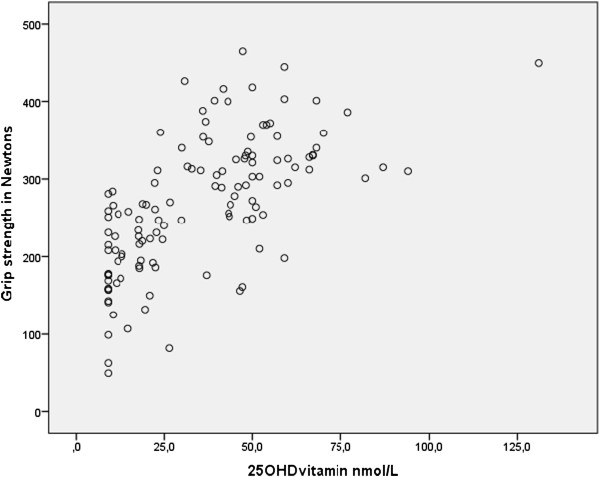
Somali participants (35%) had 25(OH)D levels of <10 nmol/L, and 90% had <25 nmol/L; 10% of Swedish participants had <25 nmol/L of 25(OH)D, and 54% had <50 nmol/L. Somali women had a relatively weak grip strength compared with Swedish women: median 202 N (inter-quartile range 167-246) vs. median 316 N (inter-quartile range 278-359), respectively. Somali women were also weak in upper leg performance: 73% were unable to squat, 29% unable to stand on one leg, and 21% could not lift their hips (not significant across 25(OH)D categories); most Swedish women could perform these tests. In the final model, grip strength (N) was significantly associated with 25(OH)D levels (B 0.94, p=0.013) together with Somali birth (B -63.9, p<0.001), age (B 2.5, p=0.02) and height (B 2.6, p=0.01).
Many Somali women had undetectable/severely low 25(OH)D concentrations and pronounced hand and upper leg weakness; grip strength was strongly associated with 25(OH)D. Maternity health care personnel should be aware of this increased frequency and manage care accordingly.
严重的维生素 D 缺乏会损害肌肉力量。本研究旨在检测有隐匿性(索马里出生)和非隐匿性(瑞典出生)低水平和高水平维生素 D(25-羟维生素 D,25(OH)D)的女性的手部和腿部的身体机能,并分析其血浆 25(OH)D 浓度。
在瑞典一家产前诊所(纬度 60°N)招募了 123 名女性(58%为瑞典人)。分析血浆 25(OH)D 水平,用 nmol/L 表示,然后分为<10=未检出、10-24、25-49、50-74 或>75。测试肌肉力量:最大握力(牛顿,N),以及腿部表现(能够/不能够进行深蹲、单腿站立、从椅子上站起来和抬起臀部)。收集社会和人体测量数据。非参数统计检验了不同 25(OH)D 类别下的测试能力的差异。未检出值(<10 nmol/L)在线性相关统计中用“9”替换。使用逐步线性回归,为握力(N)的最终主效应模型计算了独立变量:出生国家、25(OH)D 水平、年龄、身高、体重、身体活动、哺乳期状况、产次和孕龄。
索马里参与者(35%)的 25(OH)D 水平<10 nmol/L,90%的<25 nmol/L;10%的瑞典参与者的 25(OH)D 水平<25 nmol/L,54%的<50 nmol/L。与瑞典女性相比,索马里女性的握力相对较弱:中位数 202 N(四分位距 167-246)与中位数 316 N(四分位距 278-359)相比。索马里女性的腿部表现也较弱:73%的人无法深蹲,29%的人无法单腿站立,21%的人无法抬起臀部(25(OH)D 类别之间无显著差异);大多数瑞典女性可以进行这些测试。在最终模型中,握力(N)与 25(OH)D 水平(B 0.94,p=0.013)以及索马里出生(B-63.9,p<0.001)、年龄(B 2.5,p=0.02)和身高(B 2.6,p=0.01)显著相关。
许多索马里女性的 25(OH)D 浓度未检出/严重偏低,手部和腿部明显无力;握力与 25(OH)D 密切相关。产妇保健医务人员应注意到这种发病率的增加,并相应地进行管理。