Department of Physical Therapy, Faculty of Medicine, University of British Columbia (UBC), Vancouver, BC, Canada.
BMC Musculoskelet Disord. 2013 Dec 24;14:367. doi: 10.1186/1471-2474-14-367.
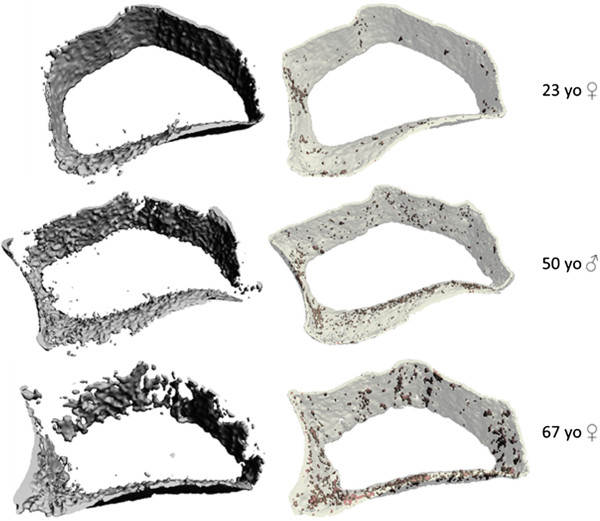
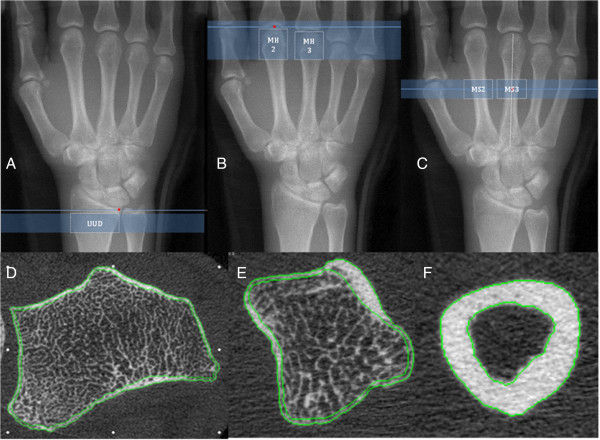
High Resolution-Peripheral Quantitative Computed Tomography (HR-pQCT) is an emerging technology for evaluation of bone quality in Rheumatoid Arthritis (RA). However, there are limitations with standard HR-pQCT imaging protocols for examination of regions of bone commonly affected in RA. We developed a customized protocol for evaluation of volumetric bone mineral density (vBMD) and microstructure at the metacarpal head (MH), metacarpal shaft (MS) and ultra-ultra-distal (UUD) radius; three sites commonly affected in RA. The purpose was to evaluate short-term measurement precision for bone density and microstructure at these sites.
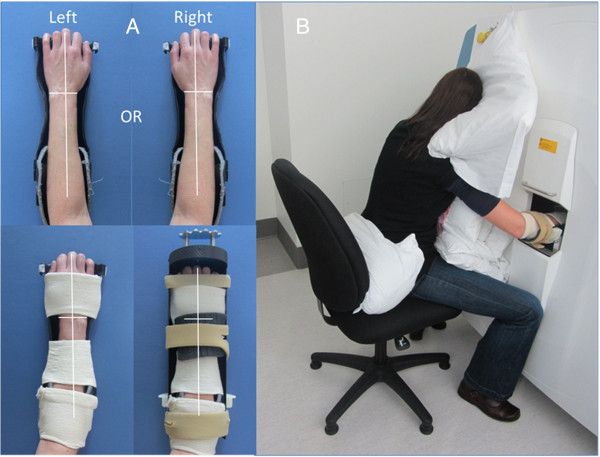
12 non-RA participants, individuals likely to have no pre-existing bone damage, consented to participate [8 females, aged 23 to 71 y [median (IQR): 44 (28) y]. The custom protocol includes more comfortable/stable positioning and adapted cortical segmentation and direct transformation analysis methods. Dominant arm MH, MS and UUD radius scans were completed on day one; repeated twice (with repositioning) three to seven days later. Short-term precision for repeated measures was explored using intraclass correlational coefficient (ICC), mean coefficient of variation (CV%), root mean square coefficient of variation (RMSCV%) and least significant change (LSC%95).
Bone density and microstructure precision was excellent: ICCs varied from 0.88 (MH2 trabecular number) to .99 (MS3 polar moment of inertia); CV% varied from < 1 (MS2 vBMD) to 6 (MS3 marrow space diameter); RMSCV% varied from < 1 (MH2 full bone vBMD) to 7 (MS3 marrow space diameter); and LSC%95 varied from 2 (MS2 full bone vBMD to 21 (MS3 marrow space diameter). Cortical porosity measures were the exception; RMSCV% varying from 19 (MS3) to 42 (UUD). No scans were stopped for discomfort. 5% (5/104) were repeated due to motion during imaging. 8% (8/104) of final images had motion artifact graded > 3 on 5 point scale.
In our facility, this custom protocol extends the potential for in vivo HR-pQCT imaging to assess, with high precision, regional differences in bone quality at three sites commonly affected in RA. Our methods are easy to adopt and we recommend other users of HR-pQCT consider this protocol for further evaluations of its precision and feasibility in their imaging facilities.
高分辨率外周定量计算机断层扫描(HR-pQCT)是一种新兴的技术,可用于评估类风湿关节炎(RA)中的骨质量。然而,对于检查 RA 常见受累部位的骨,标准的 HR-pQCT 成像方案存在局限性。我们开发了一种定制方案,用于评估掌骨头部(MH)、掌骨干(MS)和超远端(UUD)桡骨的容积骨矿物质密度(vBMD)和微观结构;这三个部位是 RA 常见的受累部位。其目的是评估这些部位骨密度和微观结构的短期测量精度。
12 名非 RA 参与者(8 名女性,年龄 23 岁至 71 岁[中位数(IQR):44(28)岁])同意参加研究。该定制方案包括更舒适/稳定的定位和适应的皮质分割和直接转换分析方法。在第一天完成优势手臂 MH、MS 和 UUD 桡骨扫描;在三到七天后重复两次(重新定位)。使用组内相关系数(ICC)、平均变异系数(CV%)、均方根变异系数(RMSCV%)和最小显著变化(LSC%95)来探讨重复性测量的短期精度。
骨密度和微观结构精度非常好:ICC 从 0.88(MH2 骨小梁数量)到 0.99(MS3 极惯性矩);CV%从 <1(MS2 vBMD)到 6(MS3 骨髓腔直径);RMSCV%从 <1(MH2 全骨 vBMD)到 7(MS3 骨髓腔直径);LSC%95 从 2(MS2 全骨 vBMD)到 21(MS3 骨髓腔直径)。皮质孔隙度测量是个例外;RMSCV%从 19(MS3)到 42(UUD)。没有因不适而停止扫描。5%(5/104)因成像过程中的运动而重复。8%(8/104)的最终图像在 5 分制的运动伪影评分为 >3。
在我们的机构中,该定制方案扩展了 HR-pQCT 成像的应用潜力,可高精度评估 RA 常见受累的三个部位的骨质量区域差异。我们的方法易于采用,我们建议 HR-pQCT 的其他使用者考虑该方案,以进一步评估其在其成像设施中的精度和可行性。