Venditti Elizabeth M, Wylie-Rosett Judith, Delahanty Linda M, Mele Lisa, Hoskin Mary A, Edelstein Sharon L
Western Psychiatric Institute and Clinic, University of Pittsburgh Medical School, 3811 O'Hara Street, Pittsburgh, PA 15213, USA.
Int J Behav Nutr Phys Act. 2014 Feb 12;11:16. doi: 10.1186/1479-5868-11-16.
Individual barriers to weight loss and physical activity goals in the Diabetes Prevention Program, a randomized trial with 3.2 years average treatment duration, have not been previously reported. Evaluating barriers and the lifestyle coaching approaches used to improve adherence in a large, diverse participant cohort can inform dissemination efforts.
Lifestyle coaches documented barriers and approaches after each session (mean session attendance = 50.3 ± 21.8). Subjects were 1076 intensive lifestyle participants (mean age = 50.6 years; mean BMI = 33.9 kg/m²; 68% female, 48% non-Caucasian). Barriers and approaches used to improve adherence were ranked by the percentage of the cohort for whom they applied. Barrier groupings were also analyzed in relation to baseline demographic characteristics.
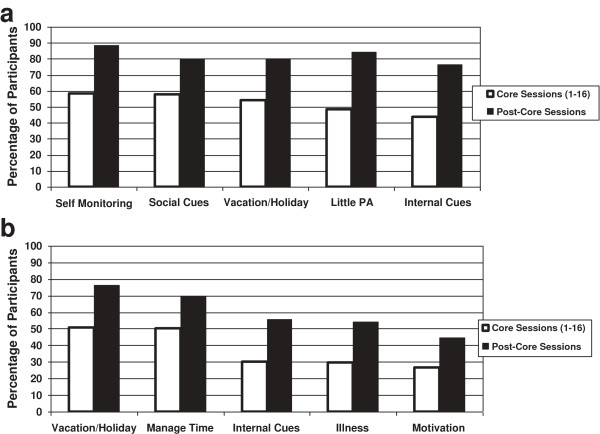
Top weight loss barriers reported were problems with self-monitoring (58%); social cues (58%); holidays (54%); low activity (48%); and internal cues (thought/mood) (44%). Top activity barriers were holidays (51%); time management (50%); internal cues (30%); illness (29%), and motivation (26%). The percentage of the cohort having any type of barrier increased over the long-term intervention period. A majority of the weight loss barriers were significantly associated with younger age, greater obesity, and non-Caucasian race/ethnicity (p-values vary). Physical activity barriers, particularly thought and mood cues, social cues and time management, physical injury or illness and access/weather, were most significantly associated with being female and obese (p < 0.001 for all). Lifestyle coaches used problem-solving with most participants (≥75% short-term; > 90% long term) and regularly reviewed self-monitoring skills. More costly approaches were used infrequently during the first 16 sessions (≤10%) but increased over 3.2 years.
Behavioral problem solving approaches have short and long term dissemination potential for many kinds of participant barriers. Given minimal resources, increased attention to training lifestyle coaches in the consistent use of these approaches appears warranted.
糖尿病预防计划是一项平均治疗时长为3.2年的随机试验,此前尚未报告过实现减肥和身体活动目标的个体障碍。评估障碍以及用于提高大型多样化参与者队列依从性的生活方式指导方法,可为推广工作提供参考。
生活方式指导人员在每次课程结束后记录障碍和方法(平均课程出席率 = 50.3 ± 21.8)。受试者为1076名强化生活方式参与者(平均年龄 = 50.6岁;平均体重指数 = 33.9 kg/m²;68%为女性,48%为非白人)。用于提高依从性的障碍和方法按适用的队列百分比进行排名。还根据基线人口统计学特征对障碍分组进行了分析。
报告的首要减肥障碍是自我监测问题(58%);社交暗示(58%);节假日(54%);活动量低(48%);以及内在暗示(思维/情绪)(44%)。首要身体活动障碍是节假日(51%);时间管理(50%);内在暗示(30%);疾病(29%)和动力(26%)。在长期干预期内存在任何类型障碍的队列百分比有所增加。大多数减肥障碍都与年龄较小、肥胖程度较高以及非白人种族显著相关(p值各不相同)。身体活动障碍,尤其是思维和情绪暗示、社交暗示和时间管理、身体损伤或疾病以及便利性 / 气候因素,与女性和肥胖最为显著相关(所有p值均 < 0.001)。生活方式指导人员对大多数参与者采用解决问题的方法(短期≥75%;长期>90%),并定期回顾自我监测技能。在最初的16次课程中,较少使用成本较高的方法(≤10%),但在3.2年期间有所增加。
行为问题解决方法对于多种参与者障碍具有短期和长期的推广潜力。鉴于资源有限,似乎有必要更加重视培训生活方式指导人员持续使用这些方法。