Infectious Diseases Research Unit, Department of Clinical Sciences in Malmö, Faculty of Medicine, Lund University, Sweden;
Infectious Diseases Research Unit, Department of Clinical Sciences in Malmö, Faculty of Medicine, Lund University, Sweden; Health Ministry, Addis Ababa, Ethiopia.
Glob Health Action. 2014 Feb 13;7:23105. doi: 10.3402/gha.v7.23105. eCollection 2014.
Currently, antiretroviral therapy (ART) is recommended for all HIV-positive patients with tuberculosis (TB). The timing of ART during the course of anti-TB treatment is based on CD4 cell counts. Access to CD4 cell testing is not universally available; this constitutes an obstacle for the provision of ART in low-income countries.
To determine clinical variables associated with HIV co-infection in TB patients and to identify correlations between clinical variables and CD4 cell strata in HIV/TB co-infected subjects, with the aim of developing a clinical scoring system for the assessment of immunosuppression.
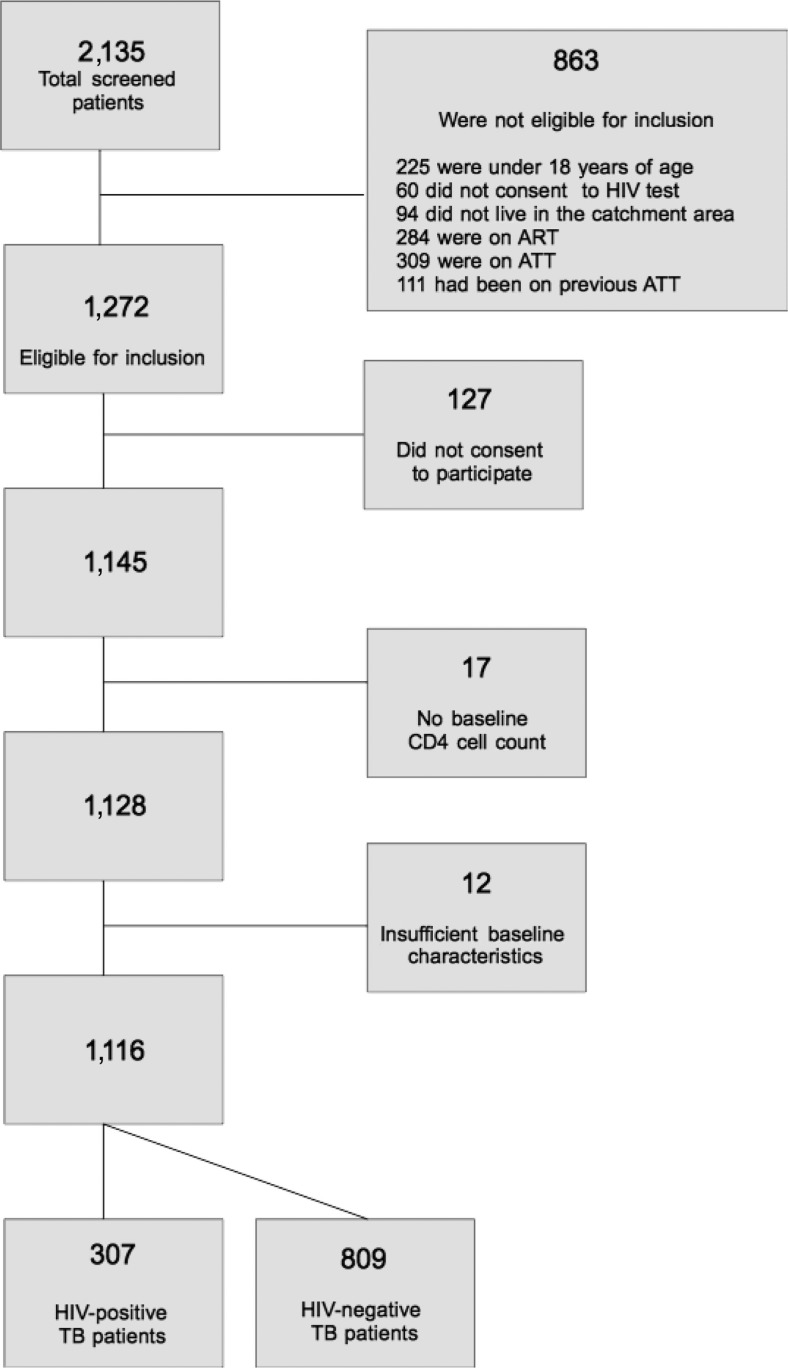
Cross-sectional study of adults with TB (with and without HIV co-infection) recruited in Ethiopian outpatient clinics. Clinical variables potentially associated with immunosuppression were recorded using a structured questionnaire, and they were correlated to CD4 cell strata used to determine timing of ART initiation. Variables found to be significant in multivariate analysis were used to construct a scoring system. Results : Among 1,116 participants, the following findings were significantly more frequent in 307 HIV-positive patients compared to 809 HIV-negative subjects: diarrhea, odynophagia, conjunctival pallor, herpes zoster, oral candidiasis, skin rash, and mid-upper arm circumference (MUAC) <20 cm. Among HIV-positive patients, conjunctival pallor, MUAC <20 cm, dyspnea, oral hairy leukoplakia (OHL), oral candidiasis, and gingivitis were significantly associated with <350 CD4 cells/mm(3). A scoring system based on these variables had a negative predictive value of 87% for excluding subjects with CD4 cell counts <100 cells/mm(3); however, the positive predictive value for identifying such individuals was low (47%).
Clinical variables correlate with CD4 cell strata in HIV-positive patients with TB. The clinical scoring system had adequate negative predictive value for excluding severe immunosuppression. Clinical scoring systems could be of use to categorize TB/HIV co-infected patients with regard to the timing of ART initiation in settings with limited access to laboratory facilities.
目前,抗逆转录病毒疗法(ART)被推荐用于所有 HIV 阳性合并结核病(TB)的患者。在抗结核治疗过程中启动 ART 的时机取决于 CD4 细胞计数。CD4 细胞检测并非普及可得,这对低收入国家提供 ART 构成了障碍。
确定与 TB 患者中 HIV 合并感染相关的临床变量,并确定 HIV/TB 合并感染患者的临床变量与 CD4 细胞分层之间的相关性,目的是开发一种用于评估免疫抑制的临床评分系统。
在埃塞俄比亚门诊诊所招募的成人 TB(伴或不伴 HIV 合并感染)患者的横断面研究。使用结构化问卷记录可能与免疫抑制相关的临床变量,并将其与用于确定 ART 启动时机的 CD4 细胞分层相关联。多变量分析中发现有统计学意义的变量被用于构建评分系统。
在 1116 名参与者中,307 名 HIV 阳性患者中以下发现明显比 809 名 HIV 阴性患者更为常见:腹泻、咽痛、结膜苍白、带状疱疹、口腔念珠菌病、皮疹和中上臂围(MUAC)<20cm。在 HIV 阳性患者中,结膜苍白、MUAC<20cm、呼吸困难、口腔毛状白斑(OHL)、口腔念珠菌病和牙龈炎与<350 CD4 细胞/mm3显著相关。基于这些变量的评分系统对排除 CD4 细胞计数<100 细胞/mm3的患者具有 87%的阴性预测值;然而,其对识别这些个体的阳性预测值较低(47%)。
临床变量与 HIV 阳性合并结核病患者的 CD4 细胞分层相关。临床评分系统对排除严重免疫抑制具有足够的阴性预测值。在实验室设施有限的情况下,临床评分系统可用于对 TB/HIV 合并感染患者进行分类,以确定 ART 启动的时机。