Department of Colorectal Surgery, Oxford University Hospitals, Churchill Hospital, Old Road, Oxford, OX3 7LJ, Headington, UK,
Surg Endosc. 2014 Jul;28(7):2221-6. doi: 10.1007/s00464-014-3432-y. Epub 2014 Feb 25.
Anastomotic leakage is a devastating complication of colorectal surgery. However, there is no technology indicative of in situ perfusion of a laparoscopic colorectal anastomosis.
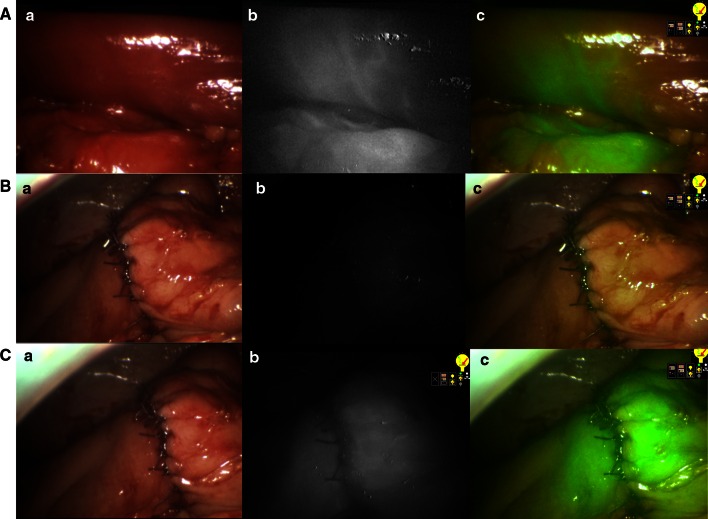
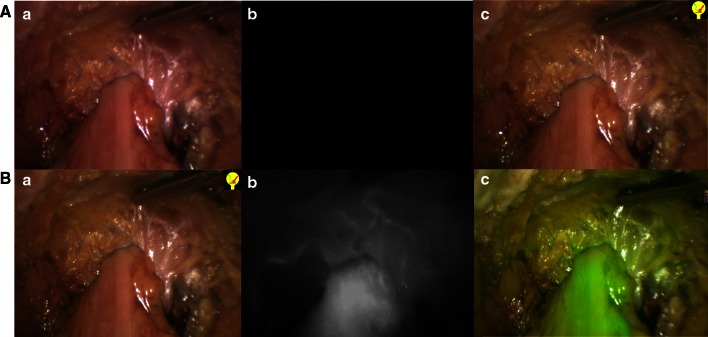
We detail the use of near-infrared (NIR) laparoscopy (PinPoint System, NOVADAQ, Canada) in association with fluorophore [indocyanine green (ICG), 2.5 mg/ml] injection in 30 consecutive patients who underwent elective minimally invasive colorectal resection using the simultaneous appearance of the cecum or distal ileum as positive control.
The median (range) age of the patients was 64 (40-81) years with a median (range) BMI of 26.7 (20-35.5) kg/m(2). Twenty-four patients had left-sided resections (including six low anterior resections) and six had right-sided resections. Of the total, 25 operations were cancer resections and five were for benign disease [either diverticular strictures (n = 3) or Crohn's disease (n = 2)]. A high-quality intraoperative ICG angiogram was achieved in 29/30 patients. After ICG injection, median (range) time to perfusion fluorescence was 35 (15-45) s. Median (range) added time for the technique was 5 (3-9) min. Anastomotic perfusion was documented as satisfactory in every successful case and encouraged avoidance of defunctioning stomas in three patients with low anastomoses. There were no postoperative anastomotic leaks.
Perfusion angiography of colorectal anastomosis at the time of their laparoscopic construction is feasible and readily achievable with minimal added intraoperative time. Further work is required to determine optimum sensitivity and threshold levels for assessment of perfusion sufficiency, in particular with regard to anastomotic viability.
吻合口漏是结直肠手术后一种毁灭性的并发症。然而,目前还没有能够指示腹腔镜结直肠吻合术原位灌注的技术。
我们详细介绍了近红外(NIR)腹腔镜(PinPoint 系统,NOVADAQ,加拿大)与荧光剂(吲哚菁绿[ICG],2.5mg/ml)注射联合使用的情况,共 30 例连续接受择期微创结直肠切除术的患者,以盲肠或远端回肠的同时出现作为阳性对照。
患者的中位(范围)年龄为 64(40-81)岁,中位(范围)BMI 为 26.7(20-35.5)kg/m²。24 例患者行左侧切除术(包括 6 例低位前切除术),6 例患者行右侧切除术。总共有 25 例手术为癌症切除术,5 例为良性疾病[分别为憩室狭窄(n=3)或克罗恩病(n=2)]。29/30 例患者获得了高质量的术中 ICG 血管造影。ICG 注射后,灌注荧光的中位(范围)时间为 35(15-45)s。该技术的中位(范围)附加时间为 5(3-9)min。在每例成功的病例中,吻合口灌注均被证明是令人满意的,并鼓励在 3 例低位吻合的患者中避免使用结肠造口术。术后无吻合口漏。
在腹腔镜构建时对结直肠吻合进行灌注血管造影是可行的,并且可以在术中花费最少的额外时间内实现。需要进一步的工作来确定灌注充足性评估的最佳敏感性和阈值水平,特别是在涉及吻合口活力方面。