Mann Bikaramjit S, Barnieh Lianne, Tang Karen, Campbell David J T, Clement Fiona, Hemmelgarn Brenda, Tonelli Marcello, Lorenzetti Diane, Manns Braden J
Department of Medicine, University of Calgary, Calgary, Alberta, Canada.
Department of Medicine, University of Calgary, Calgary, Alberta, Canada; Interdisciplinary Chronic Disease Collaboration Team, Calgary, Alberta, Canada.
PLoS One. 2014 Mar 25;9(3):e89168. doi: 10.1371/journal.pone.0089168. eCollection 2014.
Prescription drugs are used in people with hypertension, diabetes, and cardiovascular disease to manage their illness. Patient cost sharing strategies such as copayments and deductibles are often employed to lower expenditures for prescription drug insurance plans, but the impact on health outcomes in these patients is unclear.
To determine the association between drug insurance and patient cost sharing strategies on medication adherence, clinical and economic outcomes in those with chronic diseases (defined herein as diabetes, hypertension, hypercholesterolemia, coronary artery disease, and cerebrovascular disease).
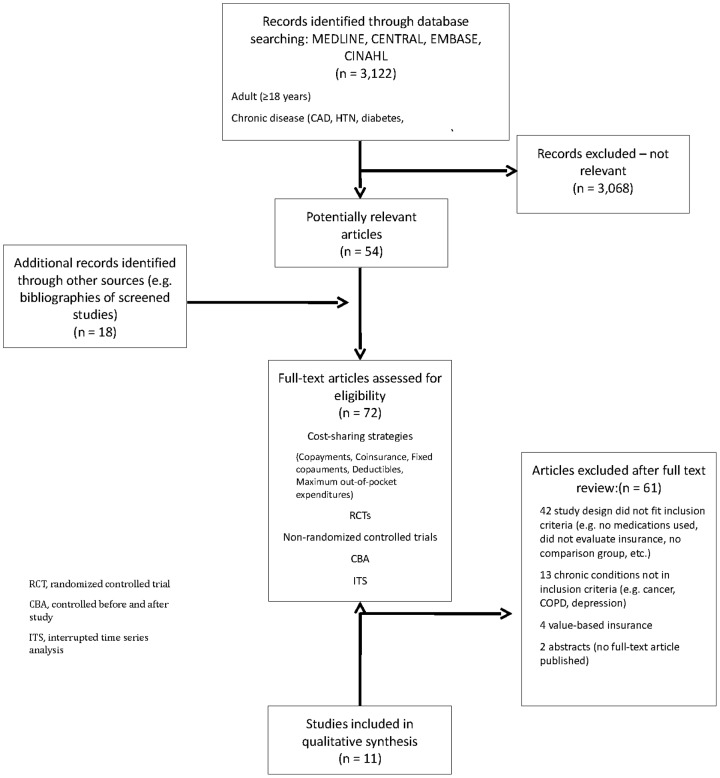
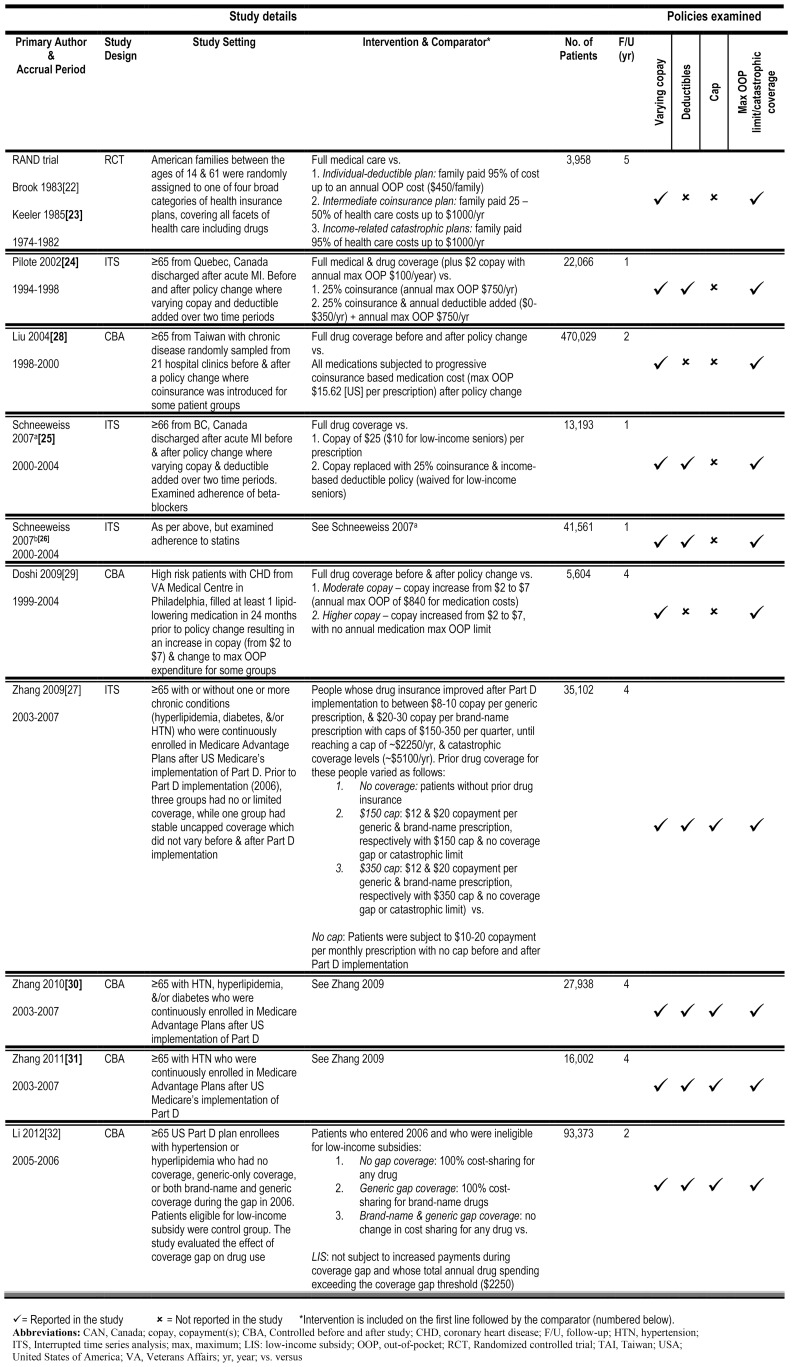
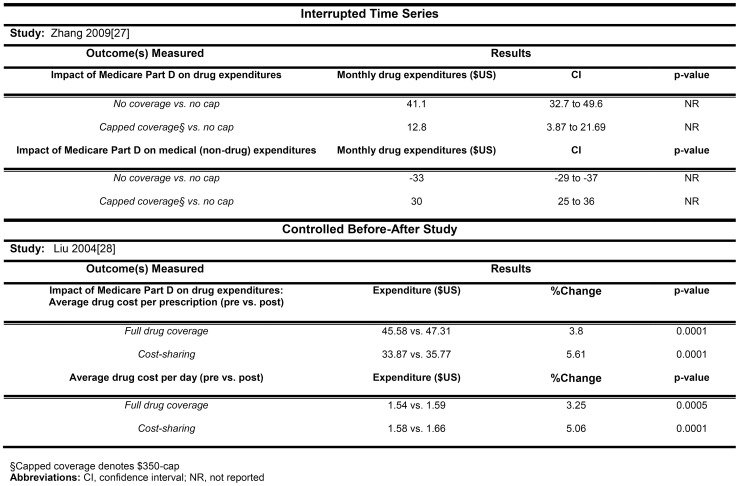
Studies were included if they examined various cost sharing strategies including copayments, coinsurance, fixed copayments, deductibles and maximum out-of-pocket expenditures. Value-based insurance design and reference based pricing studies were excluded. Two reviewers independently identified original intervention studies (randomized controlled trials, interrupted time series, and controlled before-after designs). MEDLINE, EMBASE, Cochrane Library, CINAHL, and relevant reference lists were searched until March 2013. Two reviewers independently assessed studies for inclusion, quality, and extracted data. Eleven studies, assessing the impact of seven policy changes, were included: 2 separate reports of one randomized controlled trial, 4 interrupted time series, and 5 controlled before-after studies.
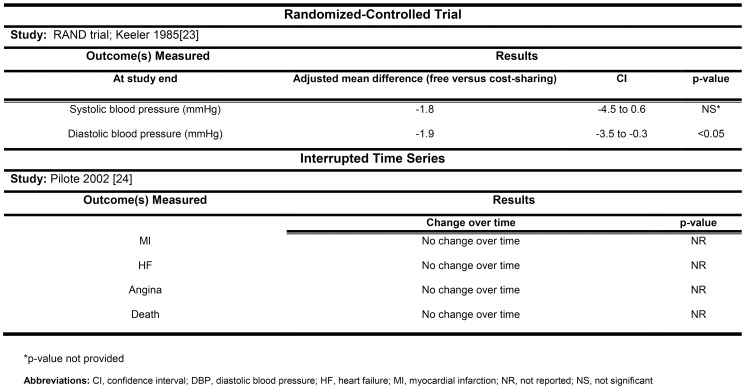
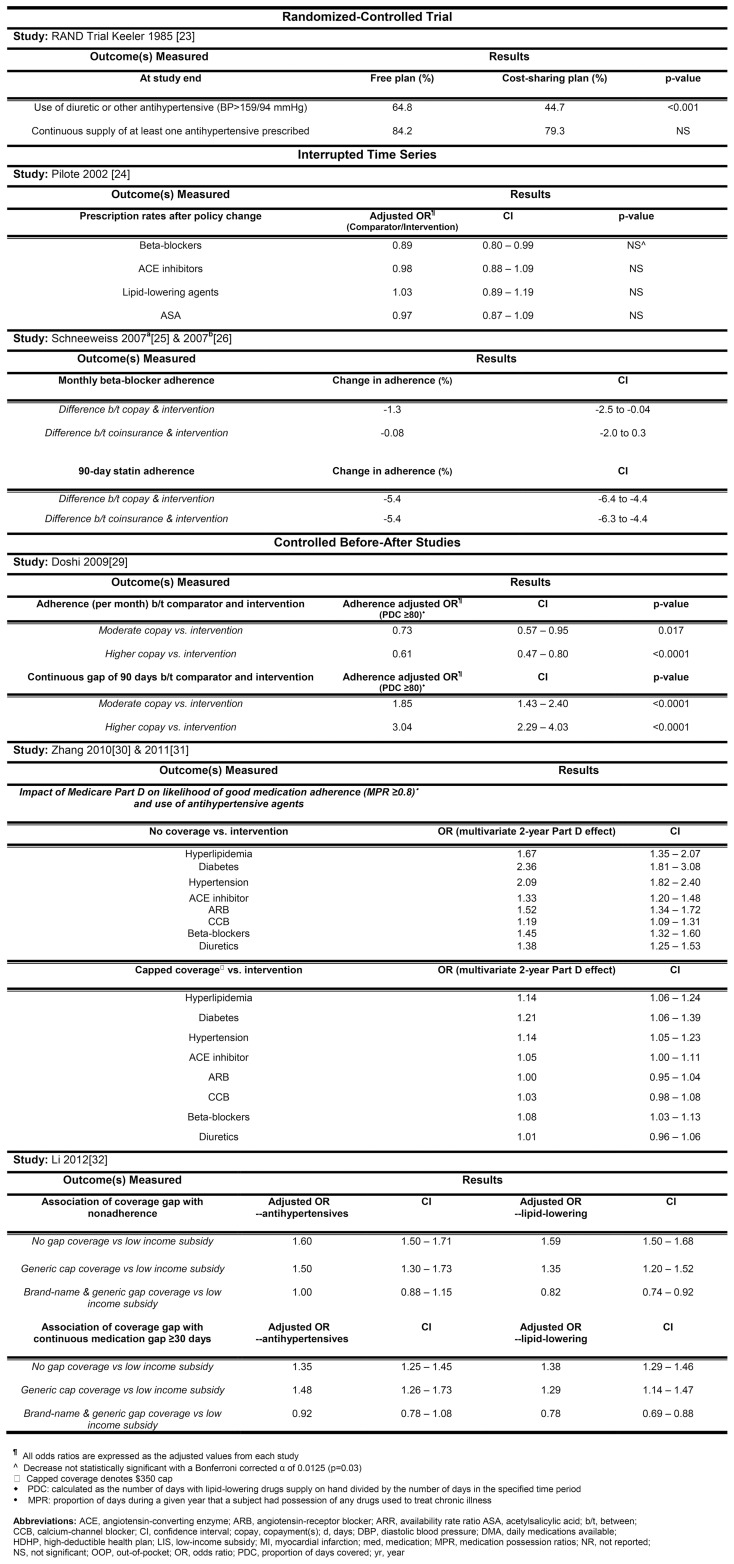
Outcomes included medication adherence, clinical events (myocardial infarction, stroke, death), quality of life, healthcare utilization, or cost. The heterogeneity among the studies precluded meta-analysis. Few studies reported the impact of cost sharing strategies on mortality, clinical and economic outcomes. The association between patient copayments and medication adherence varied across studies, ranging from no difference to significantly lower adherence, depending on the amount of the copayment.
Lowering cost sharing in patients with chronic diseases may improve adherence, but the impact on clinical and economic outcomes is uncertain.
高血压、糖尿病和心血管疾病患者使用处方药来控制病情。为降低处方药保险计划的支出,常采用患者费用分担策略,如共付额和免赔额,但这些策略对这些患者健康结局的影响尚不清楚。
确定药物保险和患者费用分担策略与慢性病(本文定义为糖尿病、高血压、高胆固醇血症、冠状动脉疾病和脑血管疾病)患者的用药依从性、临床及经济结局之间的关联。
纳入研究内容为各种费用分担策略(包括共付额、 coinsurance、固定共付额、免赔额和最高自付费用)的研究。基于价值的保险设计和基于参考定价的研究被排除。两名评审员独立识别原始干预研究(随机对照试验、中断时间序列和前后对照设计)。检索MEDLINE、EMBASE、Cochrane图书馆、CINAHL及相关参考文献列表,检索截至2013年3月。两名评审员独立评估研究是否纳入、质量并提取数据。纳入11项评估七种政策变化影响的研究:一项随机对照试验的2份单独报告、4项中断时间序列研究和5项前后对照研究。
结局包括用药依从性、临床事件(心肌梗死、中风、死亡)、生活质量、医疗保健利用或费用。研究间的异质性排除了进行荟萃分析的可能。很少有研究报告费用分担策略对死亡率、临床及经济结局的影响。患者共付额与用药依从性之间的关联在不同研究中有所不同,从无差异到依从性显著降低,这取决于共付额的数额。
降低慢性病患者的费用分担可能会提高依从性,但对临床及经济结局的影响尚不确定。