Remon J, Kampanatkosol R, Kaul R R, Muraskas J K, Christensen R D, Maheshwari A
1] Division of Neonatology, Department of Pediatrics, University of Illinois at Chicago, Chicago, IL, USA [2] Center for Neonatal and Pediatric Gastrointestinal Disease, Department of Pediatrics, University of Illinois at Chicago, Chicago, IL, USA.
Department of Pediatrics, Division of Neonatology, Loyola University Stritch School of Medicine, Maywood, IL, USA.
J Perinatol. 2014 Jul;34(7):549-54. doi: 10.1038/jp.2014.52. Epub 2014 Mar 27.
Necrotizing enterocolitis (NEC) is characterized by macrophage infiltration into affected tissues. Because intestinal macrophages are derived from recruitment and in situ differentiation of blood monocytes in the gut mucosa, we hypothesized that increased recruitment of monocytes to the intestine during NEC reduces the blood monocyte concentration and that this fall in blood monocytes can be a useful biomarker for NEC.
We reviewed medical records of very-low-birth-weight (VLBW) infants treated for NEC and compared them with a matched control group comprised of infants with feeding intolerance but no signs of NEC. Clinical characteristics and absolute monocyte counts (AMCs) were recorded. Diagnostic accuracy of AMC values was tested using receiver-operator characteristics (ROC).
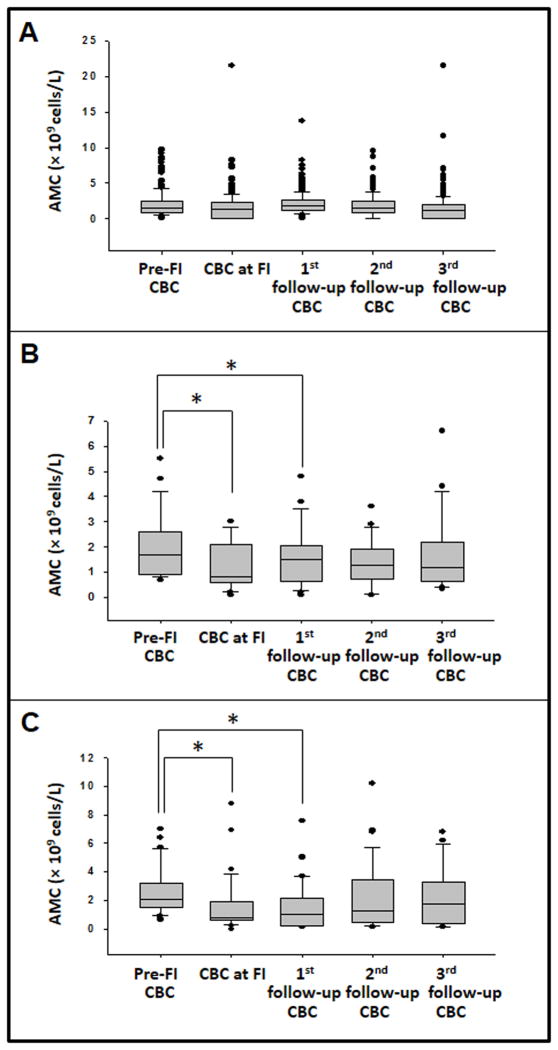
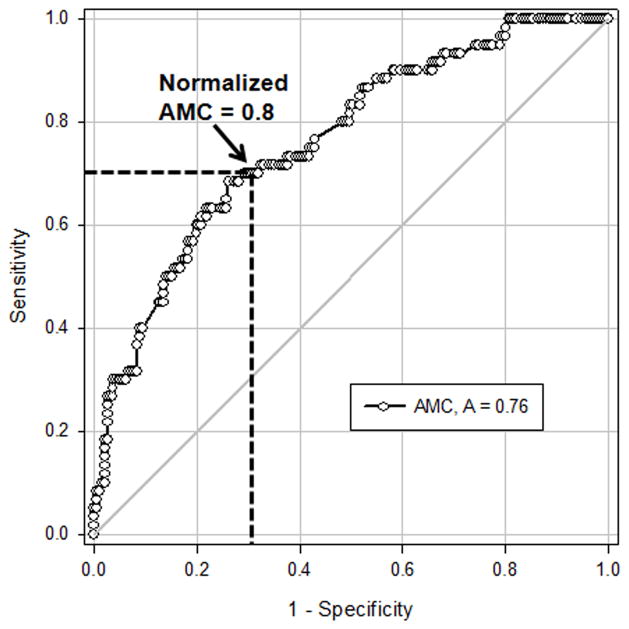
We compared 69 cases and 257 controls (median 27 weeks, range 26 to 29 in both the groups). In stage II NEC, AMCs decreased from median 1.7 × 10(9) l(-1) (interquartile range (IQR) 0.98 to 2.4) to 0.8 (IQR 0.62 to 2.1); P < 0.05. In stage III NEC, monocyte counts decreased from median 2.1 × 10(9) l(-1) (IQR 0.1.5 to 3.2) to 0.8 (IQR 0.6 to 1.9); P < 0.05. There was no change in AMCs in control infants. ROC of AMC values showed a diagnostic accuracy (area under the curve) of 0.76. In a given infant with feeding intolerance, a drop in AMCs of > 20% indicated NEC with sensitivity of 0.70 (95% confidence interval (CI) 0.57 to 0.81) and specificity of 0.71 (95% CI 0.64 to 0.77).
We have identified a fall in blood monocyte concentration as a novel biomarker for NEC in VLBW infants.
坏死性小肠结肠炎(NEC)的特征是巨噬细胞浸润至受累组织。由于肠道巨噬细胞源自肠道黏膜中血液单核细胞的募集和原位分化,我们推测在NEC期间单核细胞向肠道的募集增加会降低血液单核细胞浓度,且血液单核细胞的这种下降可能是NEC的一种有用生物标志物。
我们回顾了接受NEC治疗的极低出生体重(VLBW)婴儿的病历,并将其与由有喂养不耐受但无NEC体征的婴儿组成的匹配对照组进行比较。记录临床特征和绝对单核细胞计数(AMC)。使用受试者工作特征(ROC)曲线测试AMC值的诊断准确性。
我们比较了69例病例和257例对照(两组中位数均为27周,范围为26至29周)。在II期NEC中,AMC从中位数1.7×10⁹/L(四分位间距(IQR)0.98至2.4)降至0.8(IQR 0.62至2.1);P<0.05。在III期NEC中,单核细胞计数从中位数2.1×10⁹/L(IQR 0.1.5至3.2)降至0.8(IQR 0.6至1.9);P<0.05。对照婴儿的AMC没有变化。AMC值的ROC曲线显示诊断准确性(曲线下面积)为0.76。在给定的有喂养不耐受的婴儿中,AMC下降>20%提示NEC,敏感性为0.70(95%置信区间(CI)0.57至0.81),特异性为0.71(95%CI 0.64至0.77)。
我们已确定血液单核细胞浓度下降是VLBW婴儿NEC的一种新型生物标志物。