Thompson Douglas D, Murray Gordon D, Dennis Martin, Sudlow Cathie L M, Whiteley William N
Edinburgh MRC Hub for Trials Methodology Research, Centre for Population Health Sciences, University of Edinburgh Medical School, Teviot Place, Edinburgh EH8 9AG, UK.
BMC Med. 2014 Apr 4;12:58. doi: 10.1186/1741-7015-12-58.
The objective of this study was to: (1) systematically review the reporting and methods used in the development of clinical prediction models for recurrent stroke or myocardial infarction (MI) after ischemic stroke; (2) to meta-analyze their external performance; and (3) to compare clinical prediction models to informal clinicians' prediction in the Edinburgh Stroke Study (ESS).
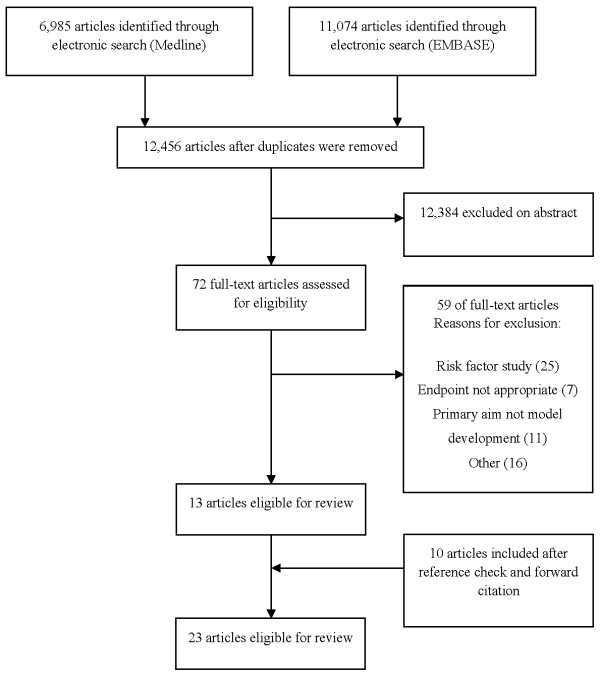
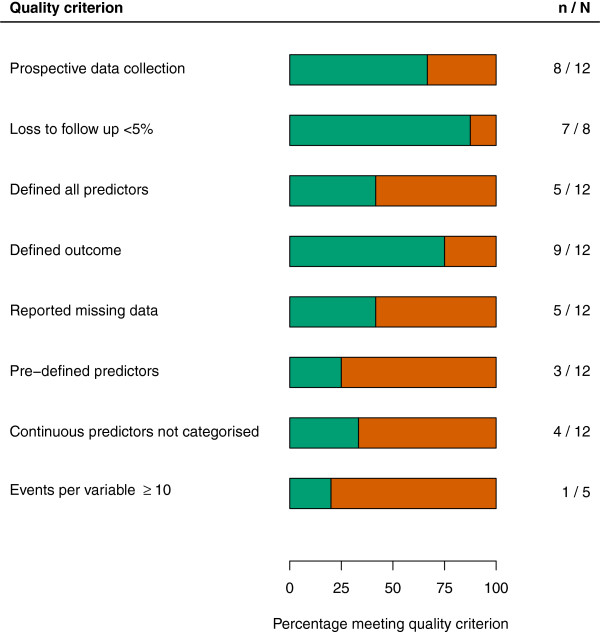
We searched Medline, EMBASE, reference lists and forward citations of relevant articles from 1980 to 19 April 2013. We included articles which developed multivariable clinical prediction models for the prediction of recurrent stroke and/or MI following ischemic stroke. We extracted information to assess aspects of model development as well as metrics of performance to determine predictive ability. Model quality was assessed against a pre-defined set of criteria. We used random-effects meta-analysis to pool performance metrics.
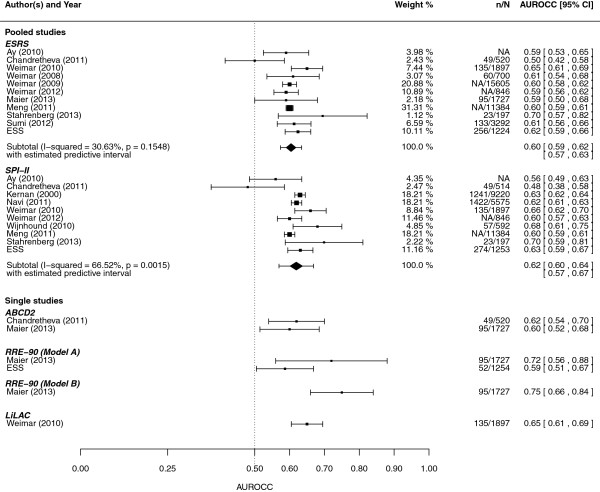
We identified twelve model development studies and eleven evaluation studies. Investigators often did not report effective sample size, regression coefficients, handling of missing data; typically categorized continuous predictors; and used data dependent methods to build models. A meta-analysis of the area under the receiver operating characteristic curve (AUROCC) was possible for the Essen Stroke Risk Score (ESRS) and for the Stroke Prognosis Instrument II (SPI-II); the pooled AUROCCs were 0.60 (95% CI 0.59 to 0.62) and 0.62 (95% CI 0.60 to 0.64), respectively. An evaluation among minor stroke patients in the ESS demonstrated that clinicians discriminated poorly between those with and those without recurrent events and that this was similar to clinical prediction models.
The available models for recurrent stroke discriminate poorly between patients with and without a recurrent stroke or MI after stroke. Models had a similar discrimination to informal clinicians' predictions. Formal prediction may be improved by addressing commonly encountered methodological problems.
本研究的目的是:(1)系统回顾缺血性卒中后复发性卒中或心肌梗死(MI)临床预测模型开发中所采用的报告内容和方法;(2)对其外部性能进行荟萃分析;(3)在爱丁堡卒中研究(ESS)中将临床预测模型与非专业临床医生的预测进行比较。
我们检索了1980年至2013年4月19日期间的Medline、EMBASE、相关文章的参考文献列表及正向引用文献。我们纳入了为预测缺血性卒中后复发性卒中和/或MI而开发多变量临床预测模型的文章。我们提取信息以评估模型开发的各个方面以及性能指标,以确定预测能力。根据一组预先定义的标准评估模型质量。我们使用随机效应荟萃分析来汇总性能指标。
我们确定了12项模型开发研究和11项评估研究。研究人员常常未报告有效样本量、回归系数、缺失数据的处理方法;通常对连续预测变量进行分类;并使用依赖数据的方法构建模型。对于埃森卒中风险评分(ESRS)和卒中预后工具II(SPI-II),可以对受试者工作特征曲线下面积(AUROCC)进行荟萃分析;汇总的AUROCC分别为0.60(95%CI 0.59至0.62)和0.62(95%CI 0.60至0.64)。ESS中对轻度卒中患者的一项评估表明,临床医生对有复发性事件和无复发性事件的患者区分能力较差,这与临床预测模型相似。
现有的复发性卒中模型对卒中后有或无复发性卒中和MI的患者区分能力较差。模型的区分能力与非专业临床医生的预测相似。通过解决常见的方法学问题,有可能改进正式的预测。