Burotto Mauricio, Wilkerson Julia, Stein Wilfred, Motzer Robert, Bates Susan, Fojo Tito
Medical Oncology Branch, Center for Cancer Research, NCI, NIH, Bethesda, Maryland, United States of America.
Medical Oncology Branch, Center for Cancer Research, NCI, NIH, Bethesda, Maryland, United States of America; Hebrew University, Jerusalem, Israel.
PLoS One. 2014 May 5;9(5):e96316. doi: 10.1371/journal.pone.0096316. eCollection 2014.
The US FDA and the EMA have approved seven agents for the treatment of renal cell carcinoma, primarily based on differences in progression-free survival (PFS). Because PFS is an arbitrary endpoint we hypothesized that an analysis would demonstrate the growth rate of tumors remained constant at the time of RECIST-defined disease progression.
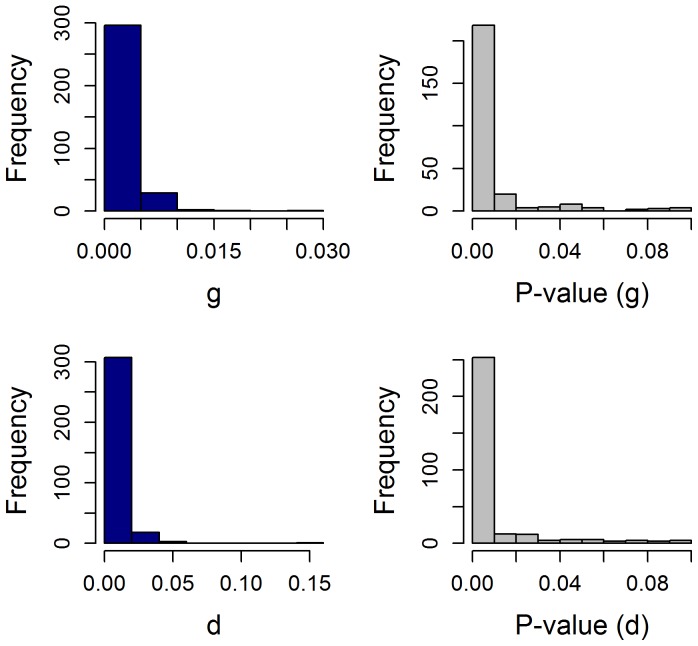
We previously estimated the growth (g) and regression (d) rates and the stability of g using data from the Phase III trial comparing sunitinib and interferon.
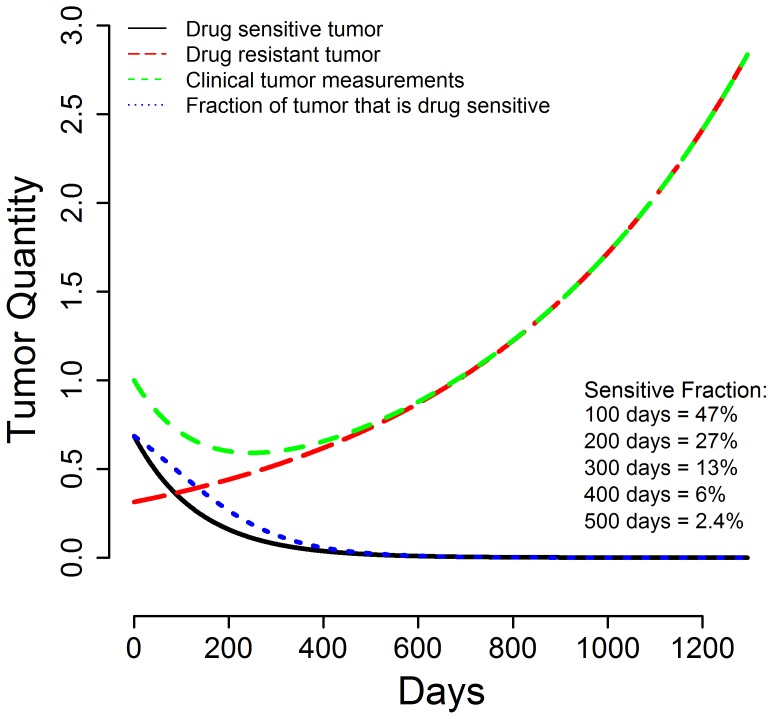
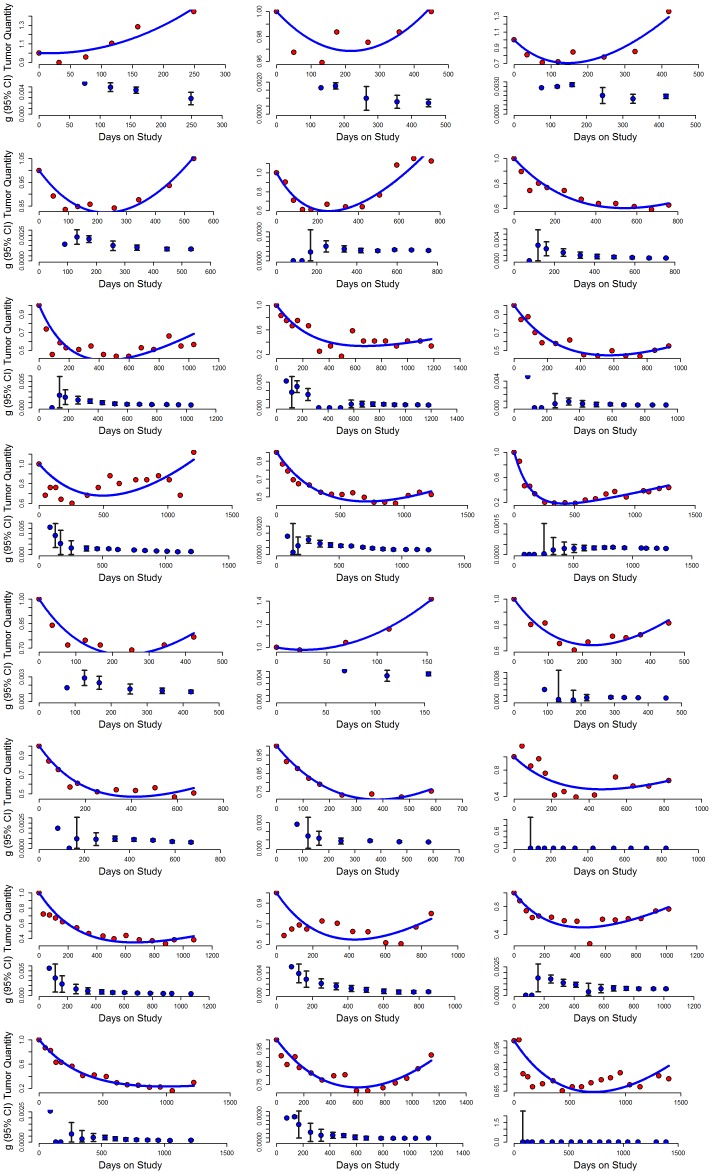
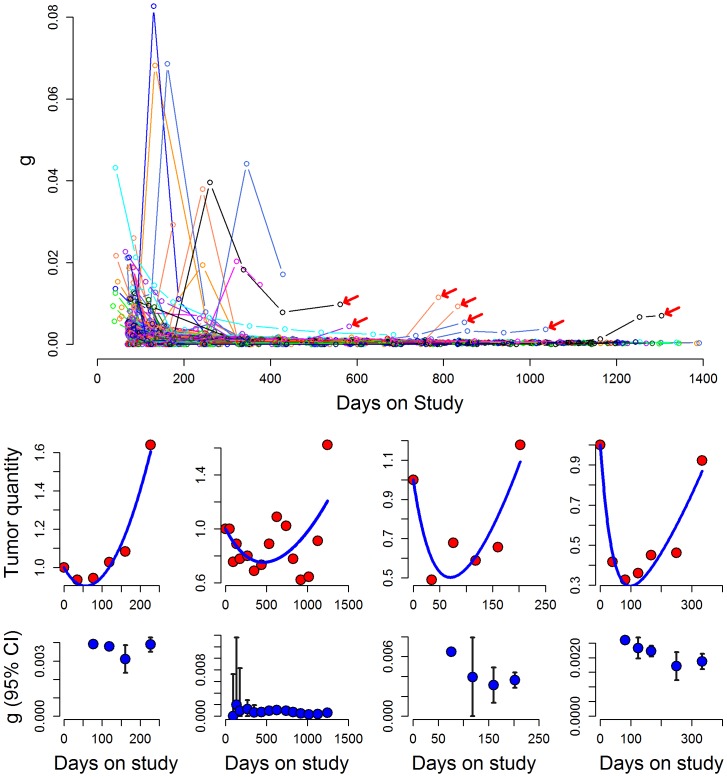
Sufficient data were available and rate constants statistically valid in 321 of 374 patients randomized to sunitinib. Median d was 0•0052 days(-1); in 53 patients no tumor growth was recorded. Median g was 0•00082 days(-1) and was stable for a median of 275 days on therapy, remaining stable beyond 300, 600 and 900 days in 122, 65 and 27 patients, respectively. A possible increase in g while receiving sunitinib could be discerned in only 18 of 321 patients. Given a median g of 0•00082 days(-1) the estimated median time to a second progression were sunitinib continued past RECIST-defined progression was 7.3 months. At 100, 200, and 300 days after starting therapy, an estimated 47%, 27%, and 13% of tumor remains sunitinib sensitive and could explain a RECIST-defined response to a new TKI.
Prolonged stability of g with sunitinib suggests continued sunitinib beyond RECIST-defined progression may provide a beneficial outcome. Randomized trials in patients whose disease has "progressed" on sunitinib are needed to test this hypothesis.
美国食品药品监督管理局(US FDA)和欧洲药品管理局(EMA)已批准了七种用于治疗肾细胞癌的药物,主要依据无进展生存期(PFS)的差异。由于PFS是一个人为设定的终点,我们推测一项分析将表明,在实体瘤疗效评价标准(RECIST)定义的疾病进展时,肿瘤的生长速率保持恒定。
我们先前使用比较舒尼替尼和干扰素的III期试验数据估计了生长(g)率和消退(d)率以及g的稳定性。
在随机接受舒尼替尼治疗的374例患者中,有321例可获得足够的数据且速率常数具有统计学有效性。中位d为0.0052天⁻¹;53例患者未记录到肿瘤生长。中位g为0.00082天⁻¹,在治疗期间中位稳定275天,分别在122例、65例和27例患者中在300天、600天和900天后仍保持稳定。在321例患者中,只有18例在接受舒尼替尼治疗时可看出g可能增加。鉴于中位g为0.00082天⁻¹,若舒尼替尼在RECIST定义的进展后继续使用,估计第二次进展的中位时间为7.3个月。在开始治疗后的100天、200天和300天,估计分别有47%、27%和13%的肿瘤对舒尼替尼敏感,这可以解释对新的酪氨酸激酶抑制剂(TKI)的RECIST定义的反应。
舒尼替尼治疗时g的长期稳定性表明,在RECIST定义的进展后继续使用舒尼替尼可能会带来有益的结果。需要对疾病在舒尼替尼治疗中已“进展”的患者进行随机试验来验证这一假设。