MacGregor E Anne
Barts Sexual Health Centre, St Bartholomew's Hospital, Centre for Neuroscience and Trauma, Blizard Institute of Cell and Molecular Science, Barts and the London School of Medicine and Dentistry, London, UK.
Int J Womens Health. 2014 May 21;6:523-35. doi: 10.2147/IJWH.S63444. eCollection 2014.
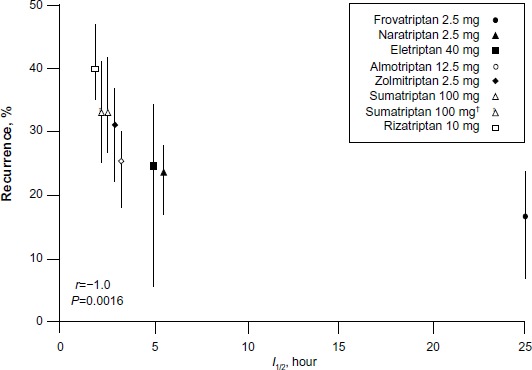
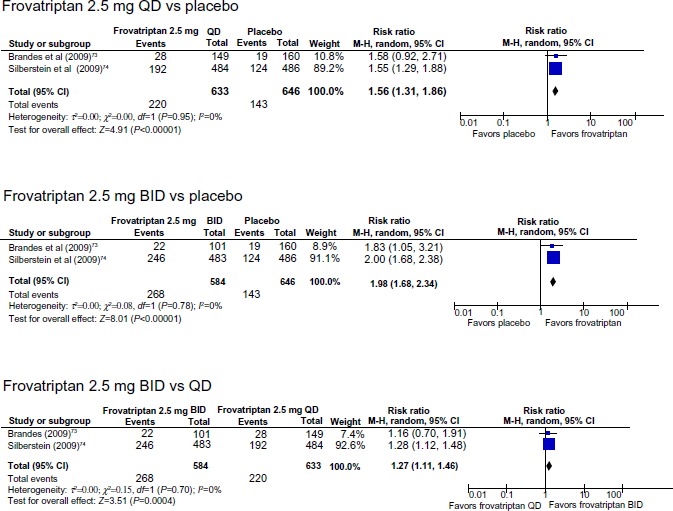
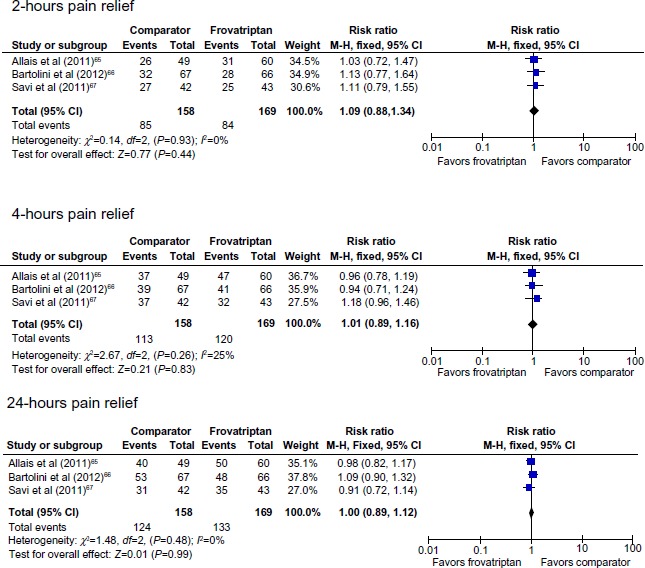
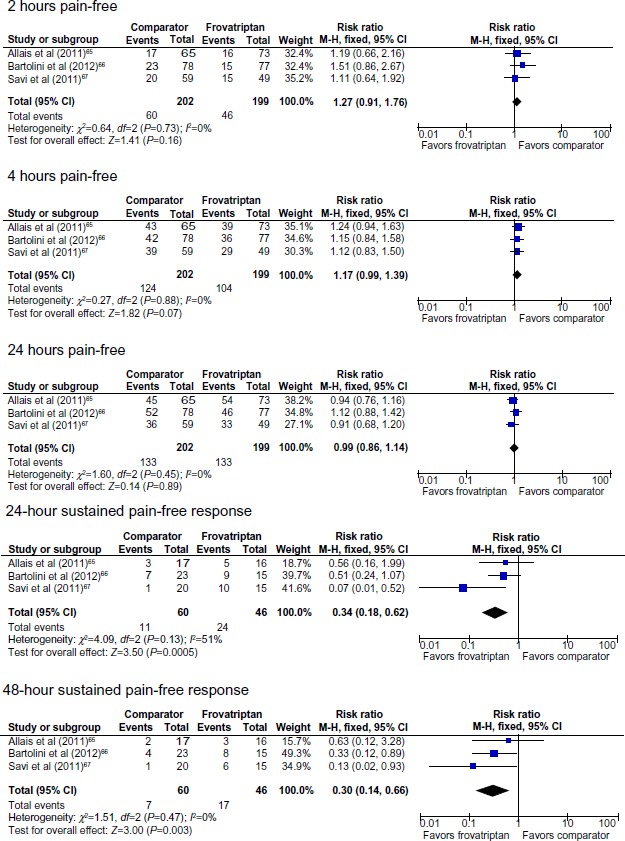
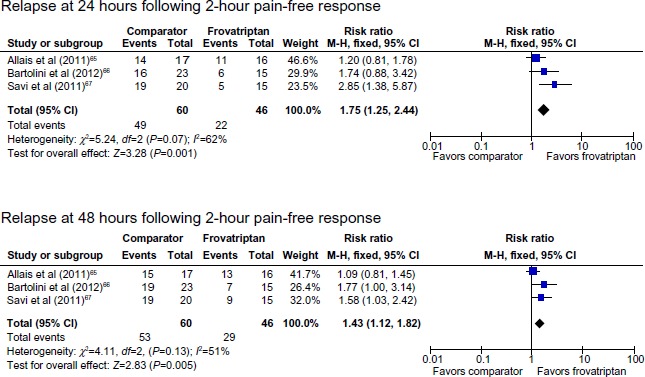
The objective of this review is to provide an overview of menstrual migraine (MM) and of frovatriptan and to assess clinical trial data regarding the efficacy and safety of frovatriptan for the acute and short-term prophylaxis of MM. Randomized controlled trials comparing frovatriptan with placebo or a triptan comparator for the acute or prophylactic treatment of MM were selected for review. MM affects up to 60% of women with migraine. Compared with attacks at other times of the cycle, menstrual attacks are longer, more severe, less responsive to treatment, more likely to relapse, and more disabling than attacks at other times of the cycle. No drugs are licensed for acute treatment of MM; triptans are recommended for treatment of moderate to severe attacks for menstrual and nonmenstrual attacks. Perimenstrual prophylaxis is indicated for patients with predictable MM that does not respond to symptomatic treatment alone. Treatment is unlicensed, but options include triptans, nonsteroidal anti-inflammatory drugs, and hormone manipulation. Frovatriptan is distinctive from other triptans due to its long elimination half-life of 26 hours, which confers a longer duration of action. Post hoc analyses from randomized trials of MM show similar pain relief and pain-free rates for frovatriptan compared with other triptans (2 hours pain-free: relative risk [RR] 1.27, 95% confidence interval [CI] 0.91-1.76) but significantly lower relapse rates (24 hours sustained pain-free: RR 0.34, 95% CI 0.18-0.62). Data from randomized controlled trials show a significant reduction in risk of MM in women using frovatriptan 2.5 mg once daily (RR 1.56, 95% CI 1.31-1.86) or twice daily (RR 1.98, 95% CI 1.68-2.34) for perimenstrual prophylaxis compared with placebo. The twice daily dosing was more effective than once daily (RR 1.27, 95% CI 1.11-1.46). These findings support the use of frovatriptan as a first-line acute treatment for MM and for perimenstrual prophylaxis.
本综述的目的是概述月经性偏头痛(MM)和夫罗曲普坦,并评估关于夫罗曲普坦用于MM急性发作和短期预防的疗效及安全性的临床试验数据。我们选择了比较夫罗曲普坦与安慰剂或其他曲坦类药物用于MM急性发作或预防性治疗的随机对照试验进行综述。MM影响高达60%的偏头痛女性。与月经周期其他时间的发作相比,月经发作持续时间更长、更严重、对治疗反应较差、更易复发,且比月经周期其他时间的发作更具致残性。目前尚无药物被批准用于MM的急性治疗;推荐使用曲坦类药物治疗月经性和非月经性发作的中重度发作。对于仅对症治疗无效的可预测性MM患者,建议进行围经期预防。治疗未获批准,但可选择的药物包括曲坦类、非甾体抗炎药和激素调控。夫罗曲普坦与其他曲坦类药物不同,因其消除半衰期长达26小时,作用持续时间更长。MM随机试验的事后分析显示,与其他曲坦类药物相比,夫罗曲普坦的疼痛缓解率和无痛率相似(2小时无痛:相对危险度[RR] 1.27,95%置信区间[CI] 0.91 - 1.76),但复发率显著更低(24小时持续无痛:RR 0.34,95% CI 0.18 - 0.62)。随机对照试验数据显示,与安慰剂相比,每日一次使用2.5 mg夫罗曲普坦(RR 1.56,95% CI 1.31 - 1.86)或每日两次(RR 1.98,95% CI 1.68 - 2.34)进行围经期预防的女性,MM风险显著降低。每日两次给药比每日一次更有效(RR 1.27,95% CI 1.11 - 1.46)。这些发现支持将夫罗曲普坦用作MM的一线急性治疗药物和围经期预防药物。