Obua Celestino, Kayiwa Joshua, Waako Paul, Tomson Göran, Balidawa Hudson, Chalker John, Ross-Degnan Dennis, Wahlstrom Rolf
Department of Pharmacology and Therapeutics, School of Biomedical Sciences, College of Health Sciences, Makerere University, Kampala, Uganda;
Data Department, Joint Clinical Research Centre, Kampala, Uganda.
Glob Health Action. 2014 Jun 4;7:24198. doi: 10.3402/gha.v7.24198. eCollection 2014.
To assess the effects of facility-based interventions using existing resources to improve overall patient attendance and adherence to antiretroviral therapy (ART) at ART-providing facilities in Uganda.
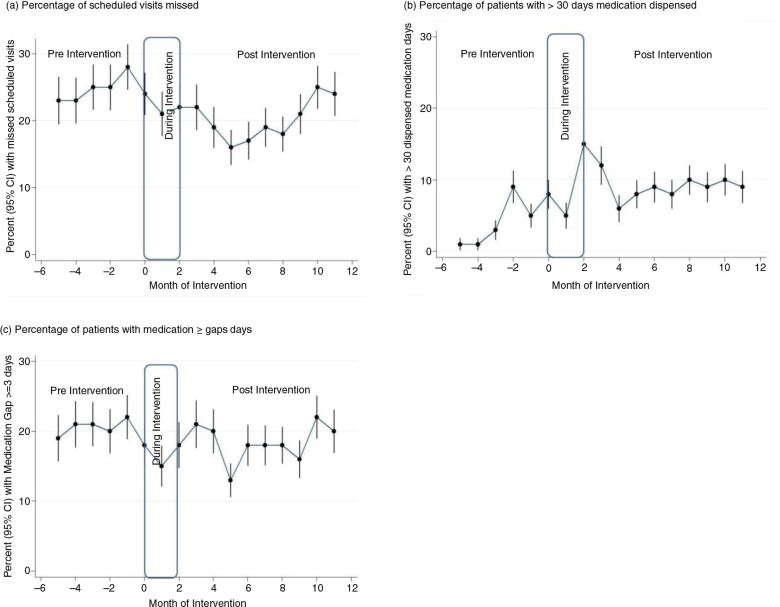
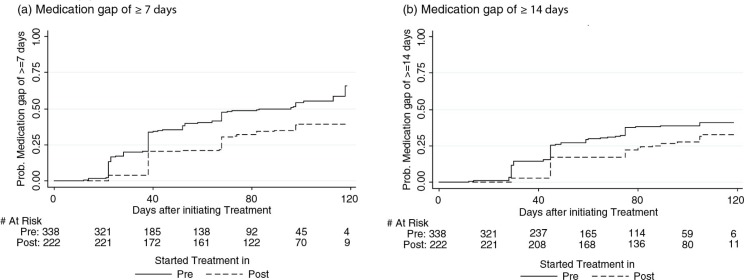
This was an interventional study which tracked attendance and treatment adherence of two distinct cohorts: experienced patients who had been on treatment for at least 12 months prior to the intervention and patients newly initiated on ART before or during the intervention. The interventions included instituting appointment system, fast-tracking, and giving longer prescriptions to experienced stable patients. Mixed-effects models were used to examine intervention effects on the experienced patients, while Cox proportional hazards models were used to determine the intervention effects on time until newly treated patients experienced gaps in medication availability.
In all, 1481 patients' files were selected for follow-up from six facilities--720 into the experienced cohort, and 761 into the newly treated cohort. Among patients in the experienced cohort, the interventions were associated with a significant reduction from 24.4 to 20.3% of missed appointments (adjusted odds ratio (AOR): 0.67; 95% confidence interval (CI): 0.59-0.77); a significant decrease from 20.2 to 18.4% in the medication gaps of three or more days (AOR: 0.69; 95% CI: 0.60-0.79); and a significant increase from 4.3 to 9.3% in the proportion of patients receiving more than 30 days of dispensed medication (AOR: 2.35; 95% CI: 1.91-2.89). Among newly treated patients, the interventions were associated with significant reductions of 44% (adjusted hazard rate (AHR): 0.56, 95% CI: 0.42-0.74) and 38% (AHR: 0.62; 95% CI: 0.45-0.85) in the hazards of experiencing a medication gap of 7 and 14 days or more, respectively.
Patients' adherence was improved with low-cost and easily implemented interventions using existing health facilities' resources. We recommend that such interventions be considered for scale-up at national levels as measures to improve clinic attendance and ART adherence among patients in Uganda and other low-resource settings in sub-Saharan Africa.
评估利用现有资源在乌干达抗逆转录病毒治疗(ART)机构开展的机构干预措施对提高患者总体就诊率及抗逆转录病毒治疗依从性的效果。
这是一项干预性研究,跟踪了两个不同队列的就诊率和治疗依从性:干预前接受治疗至少12个月的有经验患者,以及在干预前或干预期间新开始接受抗逆转录病毒治疗的患者。干预措施包括建立预约系统、快速通道服务,以及为病情稳定的有经验患者开具更长疗程的处方。采用混合效应模型检验干预措施对有经验患者的效果,同时使用Cox比例风险模型确定干预措施对新接受治疗患者出现药物供应中断时间的影响。
总共从6个机构选取了1481份患者档案进行随访——720份归入有经验队列,761份归入新接受治疗队列。在有经验队列的患者中,干预措施使失约率从24.4%显著降至20.3%(调整比值比(AOR):0.67;95%置信区间(CI):0.59 - 0.77);连续三天或更长时间的药物供应中断情况从20.2%显著降至18.4%(AOR:0.69;95% CI:0.60 - 0.79);接受超过30天配药的患者比例从4.3%显著增至9.3%(AOR:2.35;95% CI:1.91 - 2.89)。在新接受治疗的患者中,干预措施使出现7天及以上和14天及以上药物供应中断的风险分别显著降低44%(调整风险率(AHR):0.56,95% CI:0.42 - 0.74)和38%(AHR:0.62;95% CI:0.45 - 0.85)。
利用现有卫生机构资源开展低成本且易于实施的干预措施可提高患者的依从性。我们建议考虑在国家层面扩大此类干预措施,作为提高乌干达及撒哈拉以南非洲其他资源匮乏地区患者就诊率和抗逆转录病毒治疗依从性的措施。