Simon Ann M, Ingraham Kimberly A, Fey Nicholas P, Finucane Suzanne B, Lipschutz Robert D, Young Aaron J, Hargrove Levi J
Center for Bionic Medicine, Rehabilitation Institute of Chicago, Chicago, Illinois, United States of America; Department of Physical Medicine and Rehabilitation, Northwestern University, Chicago, Illinois, United States of America.
Center for Bionic Medicine, Rehabilitation Institute of Chicago, Chicago, Illinois, United States of America.
PLoS One. 2014 Jun 10;9(6):e99387. doi: 10.1371/journal.pone.0099387. eCollection 2014.
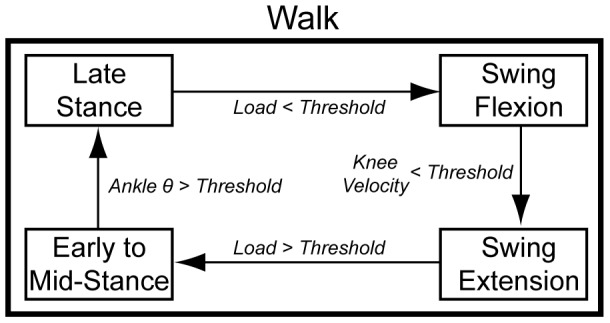
Lower limb prostheses that can generate net positive mechanical work may restore more ambulation modes to amputees. However, configuration of these devices imposes an additional burden on clinicians relative to conventional prostheses; devices for transfemoral amputees that require configuration of both a knee and an ankle joint are especially challenging. In this paper, we present an approach to configuring such powered devices. We developed modified intrinsic control strategies--which mimic the behavior of biological joints, depend on instantaneous loads within the prosthesis, or set impedance based on values from previous states, as well as a set of starting configuration parameters. We developed tables that include a list of desired clinical gait kinematics and the parameter modifications necessary to alter them. Our approach was implemented for a powered knee and ankle prosthesis in five ambulation modes (level-ground walking, ramp ascent/descent, and stair ascent/descent). The strategies and set of starting configuration parameters were developed using data from three individuals with unilateral transfemoral amputations who had previous experience using the device; this approach was then tested on three novice unilateral transfemoral amputees. Only 17% of the total number of parameters (i.e., 24 of the 140) had to be independently adjusted for each novice user to achieve all five ambulation modes and the initial accommodation period (i.e., time to configure the device for all modes) was reduced by 56%, to 5 hours or less. This approach and subsequent reduction in configuration time may help translate powered prostheses into a viable clinical option where amputees can more quickly appreciate the benefits such devices can provide.
能够产生净正机械功的下肢假肢可以为截肢者恢复更多的行走模式。然而,相对于传统假肢,这些装置的配置给临床医生带来了额外的负担;对于需要配置膝关节和踝关节的大腿截肢者使用的装置来说尤其具有挑战性。在本文中,我们提出了一种配置此类动力装置的方法。我们开发了改进的内在控制策略——这些策略模仿生物关节的行为,取决于假肢内的瞬时负荷,或者根据先前状态的值设置阻抗,以及一组起始配置参数。我们编制了表格,其中包括所需的临床步态运动学列表以及改变这些运动学所需的参数修改。我们的方法在五种行走模式(平地行走、斜坡上升/下降和楼梯上升/下降)下应用于动力膝关节和踝关节假肢。这些策略和起始配置参数集是利用三名有使用该装置经验的单侧大腿截肢者的数据开发的;然后在三名初次使用单侧大腿截肢者身上对该方法进行了测试。对于每个初次使用的用户,只需独立调整总数17%的参数(即140个参数中的24个)就能实现所有五种行走模式,并且初始适应期(即针对所有模式配置装置的时间)减少了56%,降至5小时或更短。这种方法以及随后配置时间的减少可能有助于将动力假肢转化为一种可行的临床选择,使截肢者能够更快地认识到此类装置所能带来的益处。