From the Department of Health Policy and Management, The University of North Carolina, Chapel Hill (K.H.L.); Program in Health Services and Systems Research, Duke-NUS Graduate Medical School, Singapore (Y.T., D.B.M.); Center for Health Services Research in Primary Care, Durham VAMC, NC (C.A.B., H.B.B.); VHA Health Services Research and Development Stroke Quality Enhancement Research Initiative, Indianapolis, IN (L.S.W., D.M.B.); VHA Health Services Research and Development Center of Excellence on Implementing Evidence-Based Practice, Richard L. Roudebush VHA Medical Center, Indianapolis, IN (L.S.W. D.M.B.); Regenstrief Institute, Indianapolis, IN (L.S.W., D.M.B.); Department of Veterans Affairs, Veterans Engineering Resource Center, VA-Center for Applied Systems Engineering, Indianapolis, IN (L.S.W.); Department of Internal Medicine, Indiana University School of Medicine, Indianapolis (D.M.B.); Department of Neurology, VA Greater Los Angeles Healthcare System, CA (E.M.C.); Department of Neurology, David Geffen School of Medicine, University of California, Los Angeles (E.M.C.); Department of Medicine, Division of General Internal Medicine, Duke University, Durham, NC (H.B.B., D.B.M.); Homer Consulting, Voorhees, NJ (J.B.H.); and Duke Clinical Research Institute, Duke University, Durham, NC (D.B.M.).
Stroke. 2014 Jul;45(7):2078-84. doi: 10.1161/STROKEAHA.114.004694. Epub 2014 Jun 12.
Reducing the burden of stroke is a priority for the Veterans Affairs Health System, reflected by the creation of the Veterans Affairs Stroke Quality Enhancement Research Initiative. To inform the initiative's strategic planning, we estimated the relative population-level impact and efficiency of distinct approaches to improving stroke care in the US Veteran population to inform policy and practice.
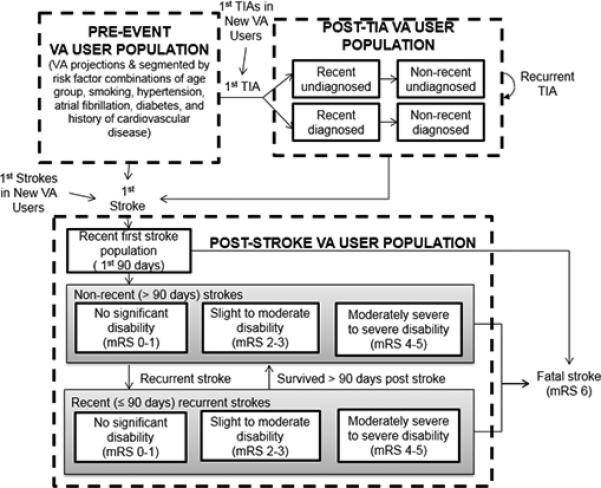
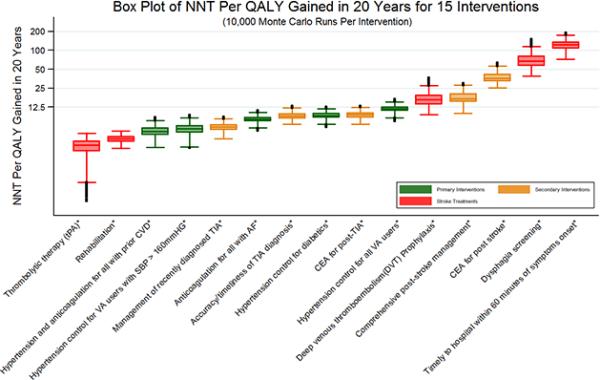
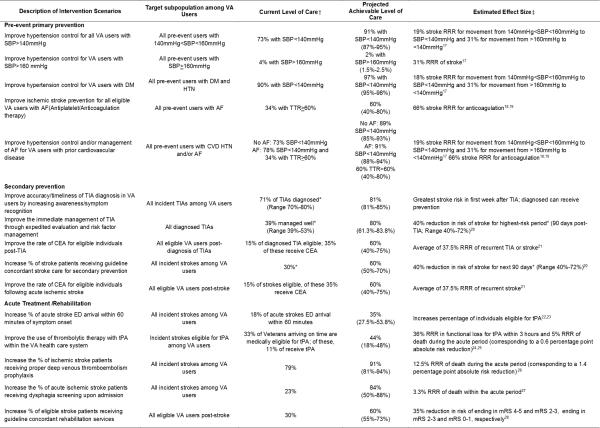
A System Dynamics stroke model of the Veteran population was constructed to evaluate the relative impact of 15 intervention scenarios including both broad and targeted primary and secondary prevention and acute care/rehabilitation on cumulative (20 years) outcomes including quality-adjusted life years (QALYs) gained, strokes prevented, stroke fatalities prevented, and the number-needed-to-treat per QALY gained.
At the population level, a broad hypertension control effort yielded the largest increase in QALYs (35,517), followed by targeted prevention addressing hypertension and anticoagulation among Veterans with prior cardiovascular disease (27,856) and hypertension control among diabetics (23,100). Adjusting QALYs gained by the number of Veterans needed to treat, thrombolytic therapy with tissue-type plasminogen activator was most efficient, needing 3.1 Veterans to be treated per QALY gained. This was followed by rehabilitation (3.9) and targeted prevention addressing hypertension and anticoagulation among those with prior cardiovascular disease (5.1). Probabilistic sensitivity analysis showed that the ranking of interventions was robust to uncertainty in input parameter values.
Prevention strategies tend to have larger population impacts, though interventions targeting specific high-risk groups tend to be more efficient in terms of number-needed-to-treat per QALY gained.
降低卒中负担是退伍军人事务部医疗体系的首要任务,这反映在退伍军人事务部卒中质量提升研究倡议的创建上。为了为该倡议的战略规划提供信息,我们评估了改善美国退伍军人卒中护理的不同方法对人群的相对影响和效率,以告知政策和实践。
构建了一个退伍军人人群的系统动力学卒中模型,以评估 15 种干预方案的相对影响,包括广泛和有针对性的一级和二级预防以及急性护理/康复对累积(20 年)结果的影响,包括获得的质量调整生命年(QALY)、预防的卒中、预防的卒中死亡以及每获得一个 QALY 需要治疗的人数。
在人群水平上,广泛的高血压控制努力产生了最大的 QALY 增加(35517),其次是针对有既往心血管疾病的退伍军人的高血压和抗凝治疗(27856)以及糖尿病患者的高血压控制(23100)。通过需要治疗的退伍军人人数来调整获得的 QALY,组织型纤溶酶原激活剂溶栓治疗的效率最高,每获得一个 QALY 需要治疗 3.1 名退伍军人。其次是康复(3.9)和针对有既往心血管疾病的退伍军人的高血压和抗凝治疗的有针对性预防(5.1)。概率敏感性分析表明,干预措施的排名对输入参数值的不确定性具有稳健性。
预防策略往往对人群的影响更大,尽管针对特定高风险人群的干预措施在每获得一个 QALY 需要治疗的人数方面效率更高。