Mohiuddin Syed, Schilder Anne, Bruce Iain
Manchester Centre for Health Economics, Institute of Population Health, University of Manchester, Oxford Road, Manchester M13 9PL, UK.
BMC Health Serv Res. 2014 Jun 13;14:253. doi: 10.1186/1472-6963-14-253.
The surgical insertion of Ventilation Tubes (VTs) for the management of persistent bilateral Otitis Media with Effusion (OME) in children remains a contentious issue due to the varying opinions regarding the risks and benefits of this procedure. The aim of this study was to evaluate the economic impact of VTs insertion for the management of persistent bilateral OME in children, providing an additional perspective on the management of one of the commonest medical conditions of childhood.
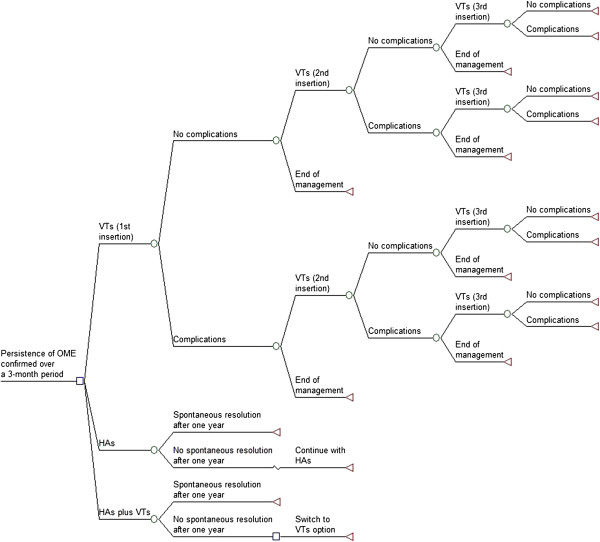
A decision-tree model was constructed to assess the cost-effectiveness of VTs strategy compared with the Hearing Aids (HAs) alone and HAs plus VTs strategies. The model used data from published sources, and assumed a 2-year time horizon and UK NHS perspective for costs. Outcomes were computed as Quality-Adjusted Life-Years (QALYs) by attaching a utility value to the total potential gains in Hearing Level in decibels (dBHL) over 12 and 24 months. Modelling uncertainty in the specification of decision-tree probabilities and QALYs was performed through Monte Carlo simulation. Expected Value of Perfect Information (EVPI) and partial EVPI (EVPPI) analyses were conducted to estimate the potential value of future research and uncertainty associated with the key parameters.
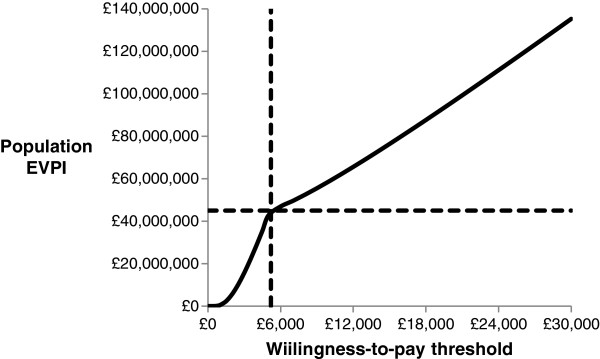
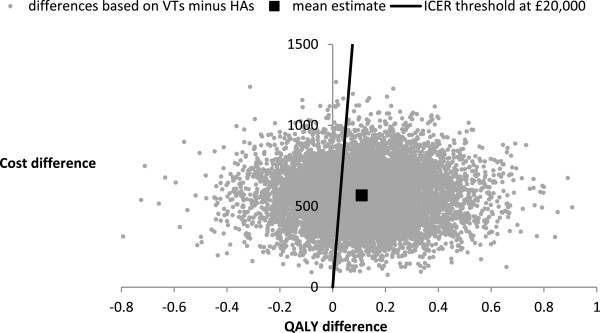
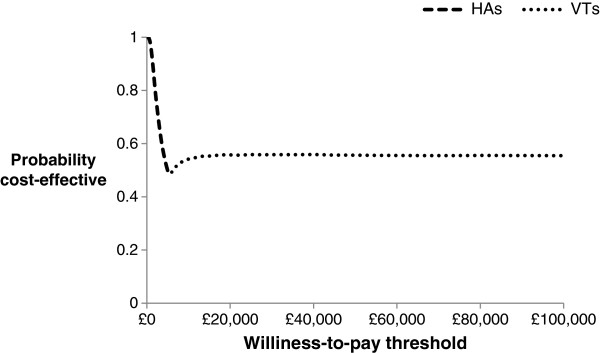
The VTs strategy was more effective and less costly when compared with the HAs plus VTs strategy, while the incremental cost-effectiveness ratio for the VTs strategy compared with the HAs strategy was £ 5,086 per QALY gained. At the willingness-to-pay threshold of £ 20,000 per QALY, the probability that the VTs strategy is likely to be more cost-effective was 0.58. The EVPI value at population level of around £ 9.5 million at the willingness-to-pay threshold of £ 20,000 indicated that future research in this area is potentially worthwhile, while the EVPPI analysis indicated considerable uncertainty surrounding the parameters used for computing the QALYs for which more precise estimates would be most valuable.
The VTs strategy is a cost-effective option when compared with the HAs alone and HAs plus VTs strategies, but the need for additional information from future study is evident to inform this surgical treatment choice. Future studies of surgical and non-surgical treatment of OME in childhood should evaluate the economic impact of pertinent interventions to provide greater context.
由于对于儿童持续性双侧中耳积液(OME)采用通气管(VT)手术置入治疗的风险和益处存在不同观点,该治疗方法仍是一个有争议的问题。本研究的目的是评估VT置入治疗儿童持续性双侧OME的经济影响,为儿童期最常见疾病之一的治疗提供另一种视角。
构建决策树模型,以评估VT策略与单独使用助听器(HA)以及HA加VT策略相比的成本效益。该模型使用已发表资料中的数据,假设时间跨度为2年,并从英国国家医疗服务体系(NHS)的角度计算成本。通过为12个月和24个月内听力水平以分贝(dBHL)为单位的总潜在增益赋予效用值,将结果计算为质量调整生命年(QALY)。通过蒙特卡洛模拟对决策树概率和QALY规格中的建模不确定性进行分析。进行完全信息期望值(EVPI)和部分EVPI(EVPPI)分析,以估计未来研究的潜在价值以及与关键参数相关的不确定性。
与HA加VT策略相比,VT策略更有效且成本更低,而与HA策略相比,VT策略的增量成本效益比为每获得一个QALY 5086英镑。在每QALY支付意愿阈值为20000英镑时,VT策略可能更具成本效益的概率为0.58。在每QALY支付意愿阈值为20000英镑时,人群水平的EVPI值约为950万英镑,这表明该领域的未来研究可能是值得的,而EVPPI分析表明,围绕用于计算QALY的参数存在相当大的不确定性,更精确的估计将最有价值。
与单独使用HA以及HA加VT策略相比,VT策略是一种具有成本效益的选择,但显然需要未来研究提供更多信息,以便为这种手术治疗选择提供依据。未来关于儿童OME手术和非手术治疗的研究应评估相关干预措施的经济影响,以提供更多背景信息。