Jiang Chunhua, Chen Jian, Liu Fuyu, Luo Yongjun, Xu Gang, Shen Hai-Ying, Gao Yuqi, Gao Wenxiang
Department of Pathophysiology and High Altitude Physiology, College of High Altitude Military Medicine, Third Military Medical University, 30 Gaotanyan Street, Shapingba District, Chongqing 400038, P,R, China.
BMC Public Health. 2014 Jul 9;14:701. doi: 10.1186/1471-2458-14-701.
Chronic mountain sickness (CMS), originally characterized by excess hemoglobin (Hb), is currently diagnosed using score-based diagnostic criteria combined with excessive erythrocytosis and clinical symptoms. However, the current criteria have limited applicability. We applied these criteria to 1,029 Chinese Han males migrated to and have been stayed at the Qinghai-Tibet plateau (3,700-5,000 m) for 2-96 months to investigate the prevalence of CMS and its correlations with Hb concentration, altitude, and the length of residence.
Subjects were screened for CMS using the latest approved diagnostic criteria combined with excessive erythrocytosis and clinical symptoms. Hb concentrations were measured, and a cut-off point was determined with k-means clustering. Predisposing factors were evaluated with binary logistic analysis and curve fitting analysis.
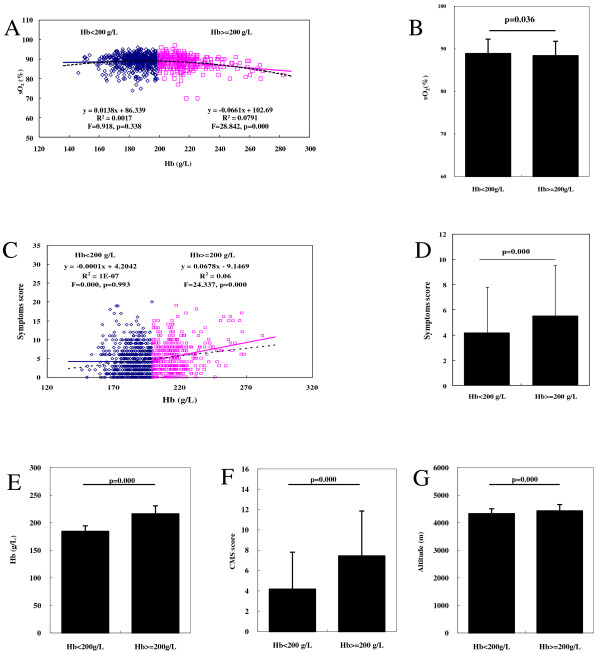
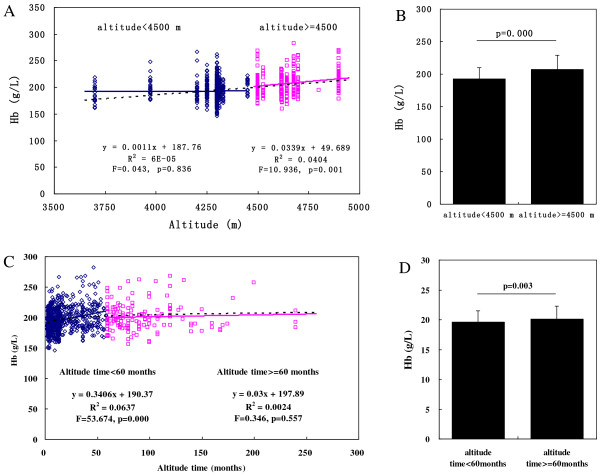
(1) The prevalence of CMS at the Qinghai-Tibetan plateau was 17.8% (183/1029 subjects, with CMS score ≥ 6, and Hb ≥ 210 g/L), which is higher than that previously reported. (2) While individuals were identified into two Hb clusters with a cut-off point of 200 g/L, in the low-Hb cluster (Hb < 200 g/L), the oxygen saturation remained stable as the Hb increased; in the high-Hb cluster (Hb ≥ 200 g/L), the oxygen saturation decreased as the Hb increased. (3) Two critical factors associated with CMS development were residence at an altitude of 4,500 m and a 60-month length of residence.
Our presenting scoring system is more sensitive than previous diagnostic criteria and favors early screening and treatment of patients with CMS. Our finding suggests that an adjusted Hb threshold of 200 g/L (instead of 210 g/L) is more adaptable in Han individuals at all altitudes. The weight of Hb level should score ≥ 6 points using the CMS scoring system because of the pathophysiologic role of excessive erythrocytosis in patients with CMS. In addition, our data suggest the importance of early screening of CMS via regular medical examinations within the first 60 months of residence at high altitudes, especially >4500 m.
慢性高原病(CMS)最初以血红蛋白(Hb)过高为特征,目前使用基于评分的诊断标准结合红细胞增多症和临床症状进行诊断。然而,当前标准的适用性有限。我们将这些标准应用于1029名移居并居住在青藏高原(海拔3700 - 5000米)2至96个月的中国汉族男性,以调查CMS的患病率及其与Hb浓度、海拔高度和居住时长的相关性。
采用最新批准的诊断标准结合红细胞增多症和临床症状对受试者进行CMS筛查。测量Hb浓度,并通过k均值聚类确定截断点。通过二元逻辑分析和曲线拟合分析评估易感因素。
(1)青藏高原地区CMS的患病率为17.8%(183/1029名受试者,CMS评分≥6且Hb≥210 g/L),高于先前报道。(2)当以200 g/L为截断点将个体分为两个Hb聚类时,在低Hb聚类(Hb < 200 g/L)中,随着Hb升高,血氧饱和度保持稳定;在高Hb聚类(Hb≥200 g/L)中,随着Hb升高,血氧饱和度下降。(3)与CMS发生相关的两个关键因素是居住在海拔4500米处和居住60个月。
我们提出的评分系统比先前的诊断标准更敏感,有利于CMS患者的早期筛查和治疗。我们的研究结果表明,调整后的Hb阈值200 g/L(而非210 g/L)在所有海拔的汉族个体中更具适应性。由于红细胞增多症在CMS患者中的病理生理作用,使用CMS评分系统时Hb水平的权重应≥6分。此外,我们的数据表明,在高海拔地区居住的前60个月内通过定期体检进行CMS早期筛查非常重要,尤其是在海拔>4500米的地区。