Wang Yingying, Freemantle Nick, Nazareth Irwin, Hunt Kate
MRC|CSO Social & Public Health Science Unit, University of Glasgow, Glasgow, United Kingdom.
Department of Primary Care and Population Health, University College London, London, United Kingdom.
PLoS One. 2014 Jul 11;9(7):e101562. doi: 10.1371/journal.pone.0101562. eCollection 2014.
To explore whether there are gender differences in the number of GP recorded cases, the probability of survival and consulting pattern prior to diagnosis amongst patients with three non-sex-specific cancers.
Cross sectional study.
UK primary care.
12,189 patients aged 16 years or over diagnosed with colorectal cancer (CRC), 11,081 patients with lung cancer and 4,352 patients with malignant melanoma, with first record of cancer diagnosis during 1997-2006.
Cancer cases recorded in primary care; probability of survival following diagnosis; and number of GP contacts within the 24 months preceding diagnosis.
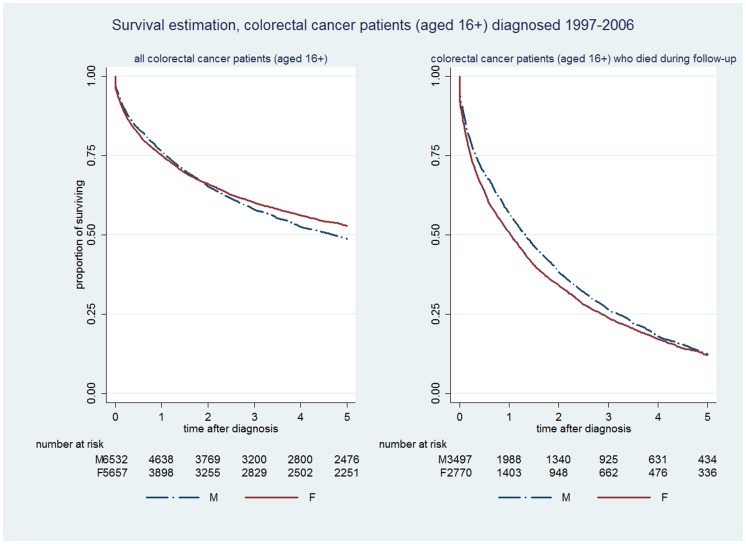
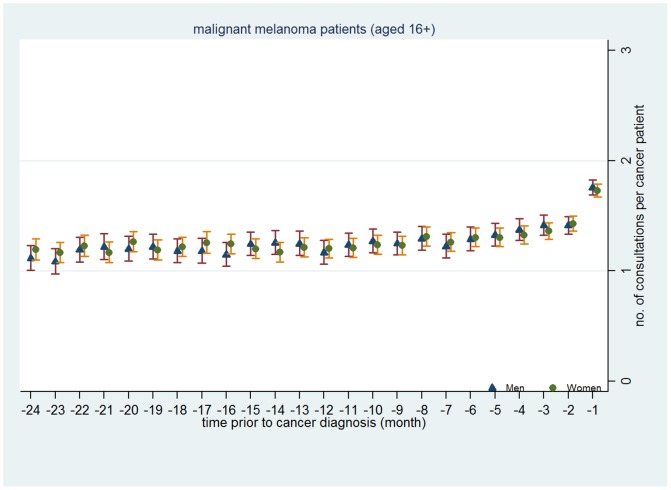
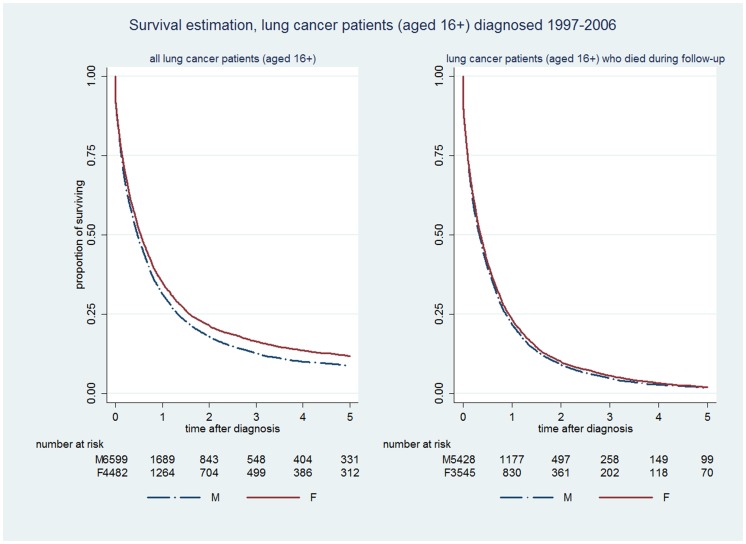
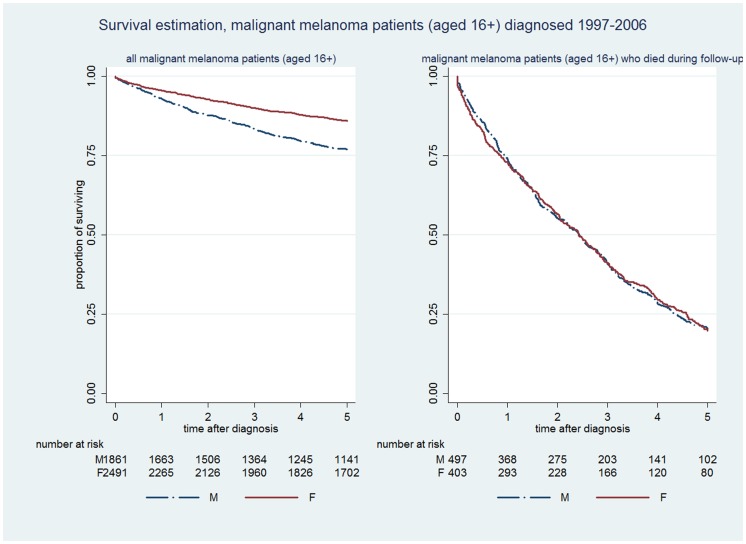
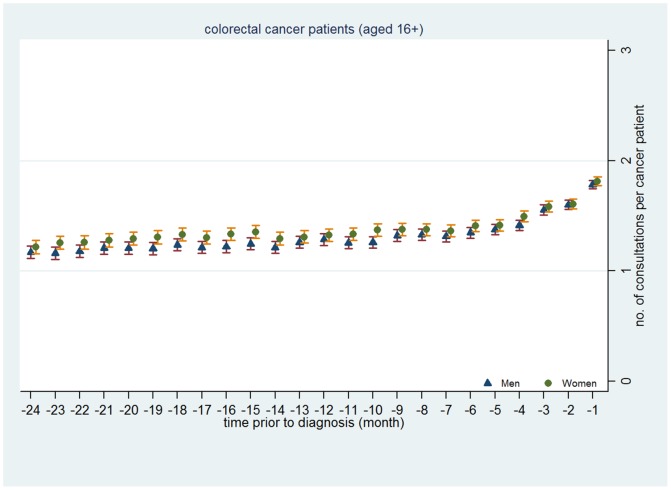
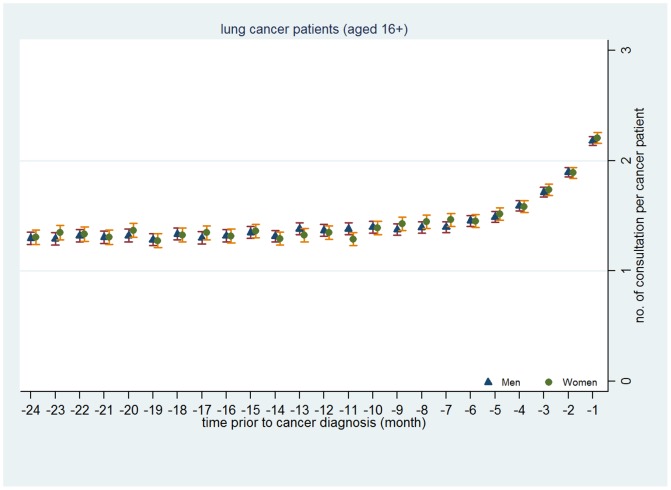
From 1997-2006, overall rates of GP recorded CRC and lung cancer cases recorded were higher in men than in women, but rates of malignant melanoma were higher in women than in men. Gender differences in survival were small; 49% of men and 53% of women survived at least 5 years following CRC diagnosis; 9% of men and 12% of women with lung cancer, and 77% of men and 86% of women with malignant melanoma. The adjusted male to female relative hazard ratio of death in all patients was 1.20 (95%CI 1.13-1.30), 1.24 (95%CI 1.16-1.33) and 1.73 (95%CI 1.51-2.00) for CRC, lung cancer and malignant melanoma respectively. However, gender differences in the relative risk were much smaller amongst those who died during follow-up. For each cancer, there was little evidence of gender difference in the percentage who consulted and the number of GP contacts made within 24 months prior to diagnosis.
This study found that patterns of consulting prior to cancer diagnosis differed little between two genders, providing no support for the hypothesis that gender differences in survival are explained by gender differences in consultation for more serious illness, and suggests the need for a more critical view of gender and consultation.
探讨三种非性别特异性癌症患者中,全科医生(GP)记录的病例数、生存概率以及诊断前的就诊模式是否存在性别差异。
横断面研究。
英国初级医疗保健机构。
1997年至2006年期间首次记录癌症诊断的12189例16岁及以上的结直肠癌(CRC)患者、11081例肺癌患者和4352例恶性黑色素瘤患者。
初级医疗保健机构记录的癌症病例;诊断后的生存概率;以及诊断前24个月内全科医生的就诊次数。
1997年至2006年期间,全科医生记录的结直肠癌和肺癌病例总数男性高于女性,但恶性黑色素瘤病例数女性高于男性。生存方面的性别差异较小;结直肠癌诊断后至少存活5年的男性为49%,女性为53%;肺癌患者中男性为9%,女性为12%;恶性黑色素瘤患者中男性为77%,女性为86%。所有患者经调整后的男性与女性死亡相对风险比,结直肠癌为1.20(95%可信区间1.13 - 1.30),肺癌为1.24(95%可信区间1.16 - 1.33),恶性黑色素瘤为1.73(95%可信区间1.51 - 2.00)。然而,在随访期间死亡的患者中,相对风险的性别差异要小得多。对于每种癌症,在诊断前24个月内就诊的百分比以及全科医生的就诊次数方面,几乎没有证据表明存在性别差异。
本研究发现,癌症诊断前的就诊模式在两性之间差异不大,这并不支持以下假设,即生存方面的性别差异是由对更严重疾病的就诊性别差异所解释的,并表明需要对性别与就诊进行更批判性的审视。