Branney Jonathan, Breen Alan C
Institute of Musculoskeletal Research & Clinical Implementation, Anglo-European College of Chiropractic, 13-15 Parkwood Road, Bournemouth BH5 2DF, UK ; The School of Health & Social Care, Bournemouth University, Royal London House, Christchurch Road, Bournemouth BH1 3LT, UK.
Institute of Musculoskeletal Research & Clinical Implementation, Anglo-European College of Chiropractic, 13-15 Parkwood Road, Bournemouth BH5 2DF, UK.
Chiropr Man Therap. 2014 Jul 1;22:24. doi: 10.1186/s12998-014-0024-9. eCollection 2014.
Spinal manipulation for nonspecific neck pain is thought to work in part by improving inter-vertebral range of motion (IV-RoM), but it is difficult to measure this or determine whether it is related to clinical outcomes.
This study undertook to determine whether cervical spine flexion and extension IV-RoM increases after a course of spinal manipulation, to explore relationships between any IV-RoM increases and clinical outcomes and to compare palpation with objective measurement in the detection of hypo-mobile segments.
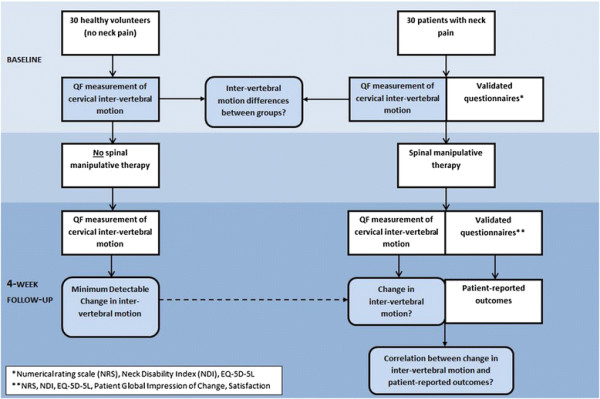
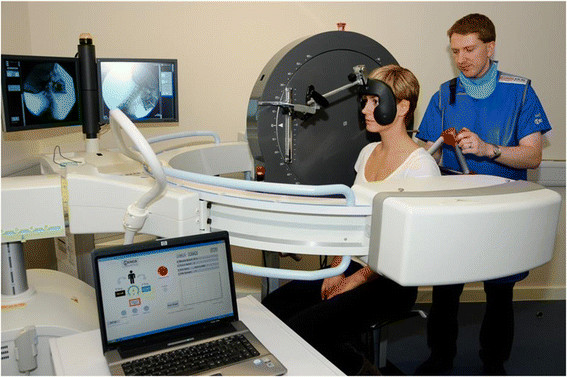
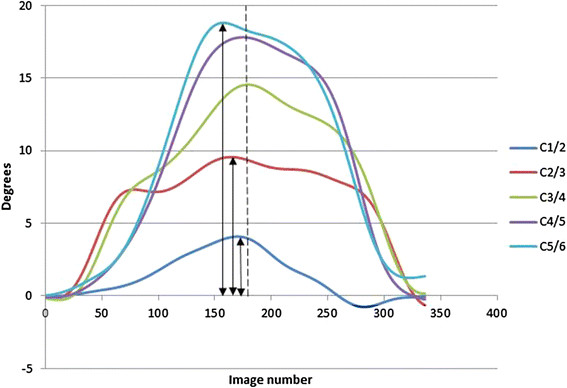
Thirty patients with nonspecific neck pain and 30 healthy controls matched for age and gender received quantitative fluoroscopy (QF) screenings to measure flexion and extension IV-RoM (C1-C6) at baseline and 4-week follow-up between September 2012-13. Patients received up to 12 neck manipulations and completed NRS, NDI and Euroqol 5D-5L at baseline, plus PGIC and satisfaction questionnaires at follow-up. IV-RoM accuracy, repeatability and hypo-mobility cut-offs were determined. Minimal detectable changes (MDC) over 4 weeks were calculated from controls. Patients and control IV-RoMs were compared at baseline as well as changes in patients over 4 weeks. Correlations between outcomes and the number of manipulations received and the agreement (Kappa) between palpated and QF-detected of hypo-mobile segments were calculated.
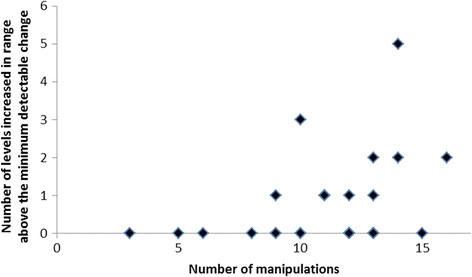
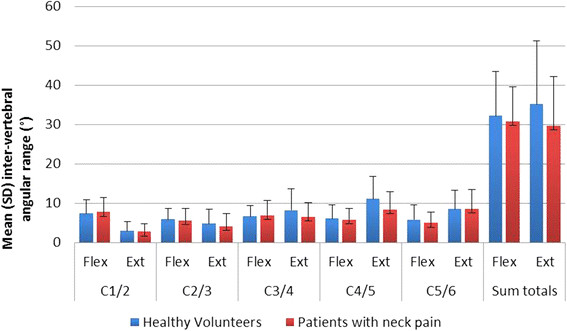
QF had high accuracy (worst RMS error 0.5o) and repeatability (highest SEM 1.1o, lowest ICC 0.90) for IV-RoM measurement. Hypo-mobility cut offs ranged from 0.8o to 3.5o. No outcome was significantly correlated with increased IV-RoM above MDC and there was no significant difference between the number of hypo-mobile segments in patients and controls at baseline or significant increases in IV-RoMs in patients. However, there was a modest and significant correlation between the number of manipulations received and the number of levels and directions whose IV-RoM increased beyond MDC (Rho=0.39, p=0.043). There was also no agreement between palpation and QF in identifying hypo-mobile segments (Kappa 0.04-0.06).
This study found no differences in cervical sagittal IV-RoM between patients with non-specific neck pain and matched controls. There was a modest dose-response relationship between the number of manipulations given and number of levels increasing IV-RoM - providing evidence that neck manipulation has a mechanical effect at segmental levels. However, patient-reported outcomes were not related to this.
脊柱推拿治疗非特异性颈部疼痛被认为部分是通过改善椎间活动范围(IV-RoM)起作用,但难以测量这一指标或确定其与临床疗效是否相关。
本研究旨在确定经过一个疗程的脊柱推拿后颈椎屈伸IV-RoM是否增加,探讨IV-RoM增加与临床疗效之间的关系,并比较触诊与客观测量在检测活动度降低节段方面的差异。
2012年9月至2013年期间,30例非特异性颈部疼痛患者和30例年龄及性别匹配的健康对照者接受了定量荧光透视(QF)检查,以测量基线及4周随访时的颈椎屈伸IV-RoM(C1-C6)。患者接受了多达12次颈部推拿,并在基线时完成了数字评分量表(NRS)、颈部残疾指数(NDI)和欧洲五维健康量表(Euroqol 5D-5L),随访时完成了患者总体印象变化量表(PGIC)和满意度问卷。确定了IV-RoM的准确性、可重复性和活动度降低的临界值。根据对照组计算了4周内的最小可检测变化(MDC)。比较了患者和对照组基线时的IV-RoM以及患者4周内的变化。计算了疗效与接受推拿次数之间的相关性以及触诊与QF检测到的活动度降低节段之间的一致性(Kappa值)。
QF测量IV-RoM具有较高的准确性(最差均方根误差0.5°)和可重复性(最高标准误1.1°,最低组内相关系数0.90)。活动度降低的临界值范围为0.8°至3.5°。没有任何疗效与高于MDC的IV-RoM增加显著相关,患者和对照组基线时活动度降低节段的数量没有显著差异,患者的IV-RoM也没有显著增加。然而,接受推拿的次数与IV-RoM增加超过MDC的节段数量和方向之间存在适度且显著的相关性(Rho=0.39,p=0.043)。在识别活动度降低节段方面,触诊与QF之间也没有一致性(Kappa值为0.04 - 0.06)。
本研究发现非特异性颈部疼痛患者与匹配的对照组之间颈椎矢状面IV-RoM没有差异。给予的推拿次数与IV-RoM增加的节段数量之间存在适度的剂量反应关系——这为颈部推拿在节段水平上具有机械效应提供了证据。然而,患者报告的疗效与此无关。