Ibáñez Raquel, Autonell Josefina, Sardà Montserrat, Crespo Nayade, Pique Pilar, Pascual Amparo, Martí Clara, Fibla Montserrat, Gutiérrez Cristina, Lloveras Belén, Moreno-Crespi Judit, Torrent Anna, Baixeras Núria, Alejo María, Bosch Francesc Xavier, de Sanjosé Silvia
Unit of Infections and Cancer; Cancer Epidemiology Research Programme, IDIBELL, Catalan Institute of Oncology (ICO), 08908 L'Hospitalet de Llobregat, Barcelona, Spain.
BMC Cancer. 2014 Aug 8;14:574. doi: 10.1186/1471-2407-14-574.
Poor attendance to cervical cancer (CC) screening is a major risk factor for CC. Efforts to capture underscreened women are considerable and once women agree to participate, the provision of longitudinal validity of the screening test is of paramount relevance. We evaluate the addition of high risk HPV test (HPV) to cervical cytology as a primary screening test among underscreened women in the longitudinal prediction of intraepithelial lesions grade 2 or worse (CIN2+).
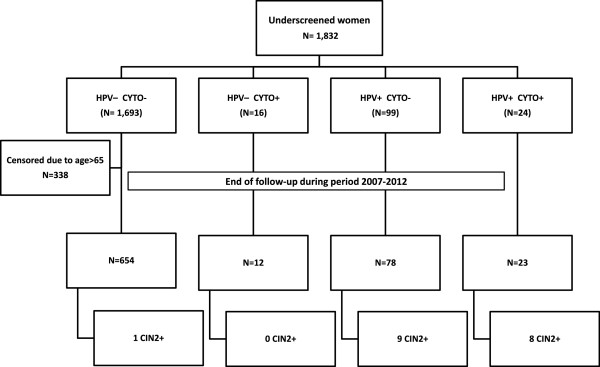
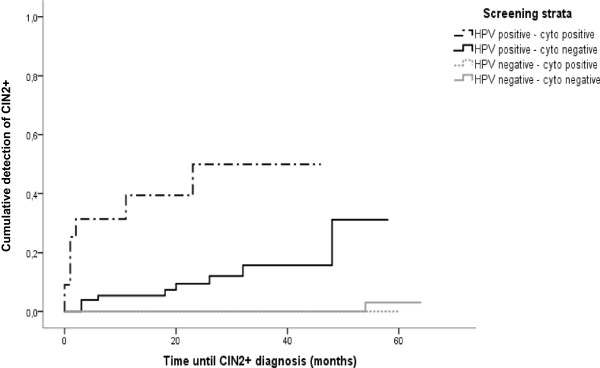
Women were included in the study if they were older than 39 years and with no evidence of cervical cytology in the previous five years within the Public Primary Health Care System in Catalonia (Spain). 1,832 underscreened women from eight public primary health areas were identified during 2007-2008 and followed-up for over three years to estimate longitudinal detection of CIN2+. Accuracy of each screening test and the combination of both to detect CIN2+ was estimated. The risk of developing CIN2+ lesions according to histology data by cytology and HPV test results at baseline was estimated using the Kaplan-Meier method.
At baseline, 6.7% of participants were HPV positive, 2.2% had an abnormal cytology and 1.3% had both tests positive. At the end of follow-up, 18 out of 767 (2.3%) underscreened women had a CIN2+, two of which were invasive CC. The three-year longitudinal sensitivity and specificity estimates to detect CIN2+ were 90.5% and 93.0% for HPV test and 38.2% and 97.8% for cytology. The negative predictive value was >99.0% for each test. No additional gains in validity parameters of HPV test were observed when adding cytology as co-test. The referral to colposcopy was higher for HPV but generated 53% higher detection of CIN2+ compared to cytology.
Underscreened women had high burden of cervical disease. Primary HPV screening followed by cytology triage could be the optimal strategy to identify CIN2+ leading to longer and safe screen intervals.
宫颈癌(CC)筛查参与率低是CC的主要危险因素。为筛查不足的女性人群开展筛查的工作力度很大,一旦女性同意参与,筛查试验的纵向有效性至关重要。我们评估在宫颈细胞学检查基础上增加高危型人乳头瘤病毒检测(HPV)作为主要筛查试验,用于纵向预测筛查不足的女性发生2级或更高级别上皮内病变(CIN2+)的情况。
纳入研究的女性年龄大于39岁,且过去五年内在西班牙加泰罗尼亚的公共初级卫生保健系统中没有宫颈细胞学检查记录。2007年至2008年期间,从八个公共初级卫生保健区域中识别出1832名筛查不足的女性,并对其进行了三年多的随访,以评估CIN2+的纵向检出情况。评估了每种筛查试验以及两者联合检测CIN2+的准确性。使用Kaplan-Meier方法根据基线时的细胞学和HPV检测结果的组织学数据估算发生CIN2+病变的风险。
基线时,6.7%的参与者HPV呈阳性,2.2%的参与者细胞学异常,1.3%的参与者两项检测均呈阳性。随访结束时,767名(2.3%)筛查不足的女性中有18例发生CIN2+,其中2例为浸润性CC。HPV检测三年纵向检测CIN2+的敏感性和特异性估计值分别为90.5%和93.0%,细胞学检测分别为38.2%和97.8%。每项检测的阴性预测值均>99.0%。将细胞学作为联合检测添加时,未观察到HPV检测有效性参数有额外提高。HPV检测转诊至阴道镜检查的比例更高,但与细胞学检测相比,CIN2+的检出率高出53%。
筛查不足的女性宫颈疾病负担较重。以HPV初筛随后进行细胞学分流可能是识别CIN2+的最佳策略,可实现更长且安全的筛查间隔。