Koshy Elizabeth, Bottle Alex, Murray Joanna, Sharland Mike, Saxena Sonia
Department of Primary Care and Public Health, Imperial College London, London, United Kingdom.
Doctor Foster Unit, Imperial College London, London, United Kingdom.
PLoS One. 2014 Aug 11;9(8):e103600. doi: 10.1371/journal.pone.0103600. eCollection 2014.
To assess whether increased awareness and diagnosis of obstructive sleep apnoea syndrome (OSAS) and national guidance on tonsillectomy for recurrent tonsillitis have influenced the socio-demographic profile of children who underwent tonsillectomy over the last decade.
Retrospective time-trends study of Hospital Episodes Statistics data. We examined the age, sex and deprivation level, alongside OSAS diagnoses, among children aged <16 years who underwent (adeno)tonsillectomy in England between 2001/2 and 2011/12.
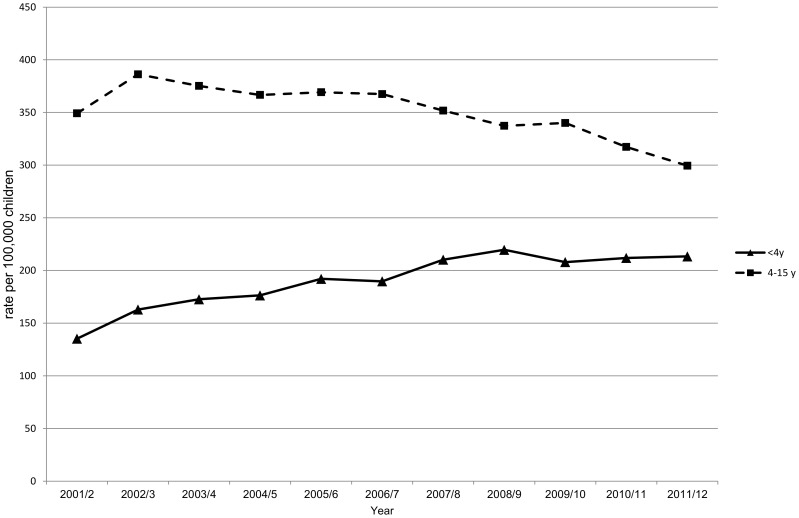
Among children aged <16 years, there were 29,697 and 27,732 (adeno)tonsillectomies performed in 2001/2 and 2011/12, respectively. The median age at (adeno)tonsillectomy decreased from 7 (IQR: 5-11) to 5 (IQR: 4-9) years over the decade. (Adeno)tonsillectomy rates among children aged 4-15 years decreased by 14% from 350 (95%CI: 346-354) in 2001/2 to 300 (95%CI: 296-303) per 100,000 children in 2011/12. However, (adeno)tonsillectomy rates among children aged <4 years increased by 58% from 135 (95%CI: 131-140) to 213 (95%CI 208-219) per 100,000 children in 2001/2 and 2011/2, respectively. OSAS diagnoses among children aged <4 years who underwent surgery increased from 18% to 39% between these study years and the proportion of children aged <4 years with OSAS from the most deprived areas increased from 5% to 12%, respectively.
(Adeno)tonsillectomy rates declined among children aged 4-15 years, which reflects national guidelines recommending the restriction of the operation to children with more severe recurrent throat infections. However, (adeno)tonsillectomy rates among pre-school children substantially increased over the past decade and one in five children undergoing the operation was aged <4 years in 2011/12.The increase in surgery rates in younger children is likely to have been driven by increased awareness and detection of OSAS, particularly among children from the most deprived areas.
评估阻塞性睡眠呼吸暂停综合征(OSAS)认知度和诊断率的提高以及复发性扁桃体炎扁桃体切除术的国家指南是否对过去十年接受扁桃体切除术的儿童的社会人口统计学特征产生了影响。
对医院病历统计数据进行回顾性时间趋势研究。我们调查了2001/2至2011/12年间在英格兰接受(腺样体)扁桃体切除术的16岁以下儿童的年龄、性别和贫困水平以及OSAS诊断情况。
在16岁以下儿童中,2001/2年和2011/12年分别进行了29,697例和27,732例(腺样体)扁桃体切除术。在这十年间,(腺样体)扁桃体切除术的中位年龄从7岁(四分位间距:5 - 11岁)降至5岁(四分位间距:4 - 9岁)。4至15岁儿童的(腺样体)扁桃体切除率从2001/2年的每10万名儿童350例(95%置信区间:346 - 354)降至2011/12年的每10万名儿童300例(95%置信区间:296 - 303),下降了14%。然而,2001/2年和2011/12年,4岁以下儿童的(腺样体)扁桃体切除率分别从每10万名儿童135例(95%置信区间:131 - 140)增至213例(95%置信区间:208 - 219),增长了58%。在这些研究年份之间,接受手术的4岁以下儿童中OSAS诊断率从18%增至39%,来自最贫困地区的4岁以下OSAS儿童比例分别从5%增至12%。
4至15岁儿童的(腺样体)扁桃体切除率下降,这反映了国家指南建议将该手术限制在复发性咽喉感染更严重的儿童中。然而,在过去十年中,学龄前儿童的(腺样体)扁桃体切除率大幅上升,2011/12年接受该手术的儿童中有五分之一年龄小于4岁。年幼儿童手术率的增加可能是由于对OSAS的认知度和检出率提高,特别是在最贫困地区的儿童中。