Inohara Taku, Kohsaka Shun, Sato Naoki, Kajimoto Katsuya, Keida Takehiko, Mizuno Masayuki, Takano Teruo
Department of Cardiology, Keio University School of Medicine, Tokyo, Japan.
Internal Medicine, Cardiology and Intensive Care Unit, Nippon Medical School Musashi-Kosugi Hospital, Kanagawa, Japan.
PLoS One. 2014 Sep 8;9(9):e105596. doi: 10.1371/journal.pone.0105596. eCollection 2014.
Renal dysfunction associated with acute decompensated heart failure (ADHF) is associated with impaired outcomes. Its mechanism is attributed to renal arterial hypoperfusion or venous congestion, but its prognostic impact based on each of these clinical profiles requires elucidation.
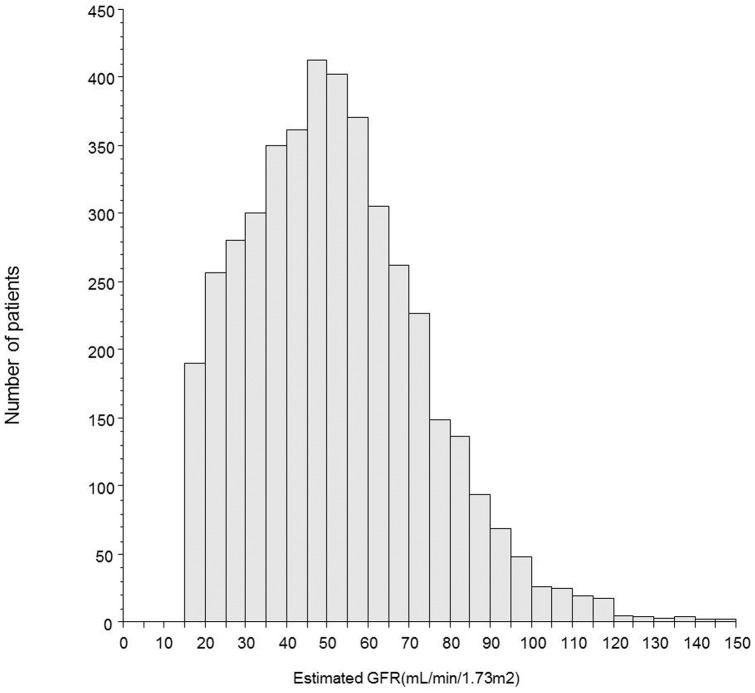
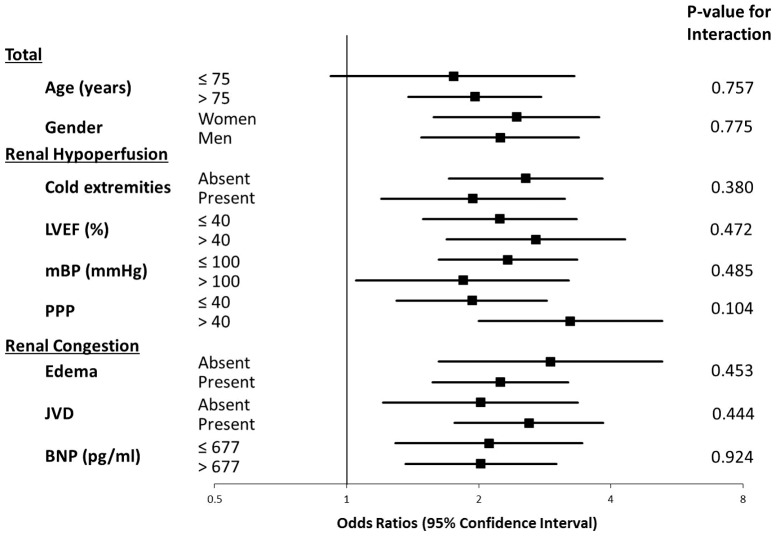
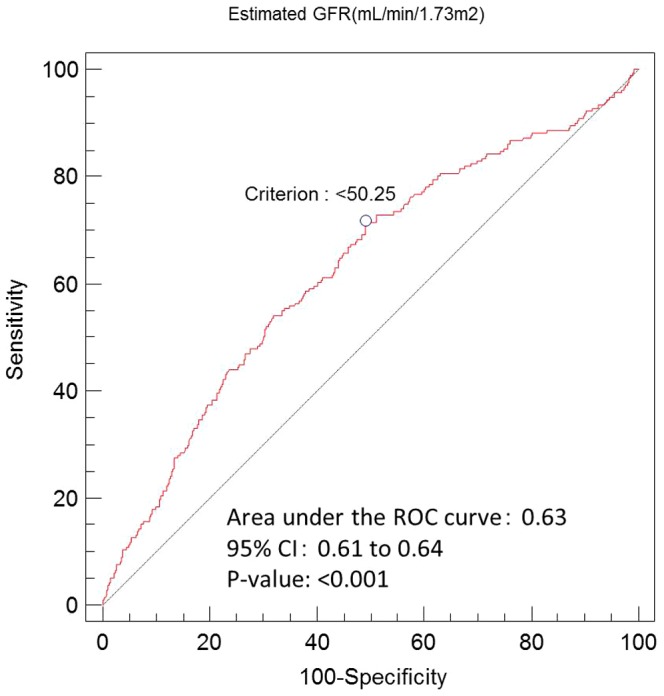
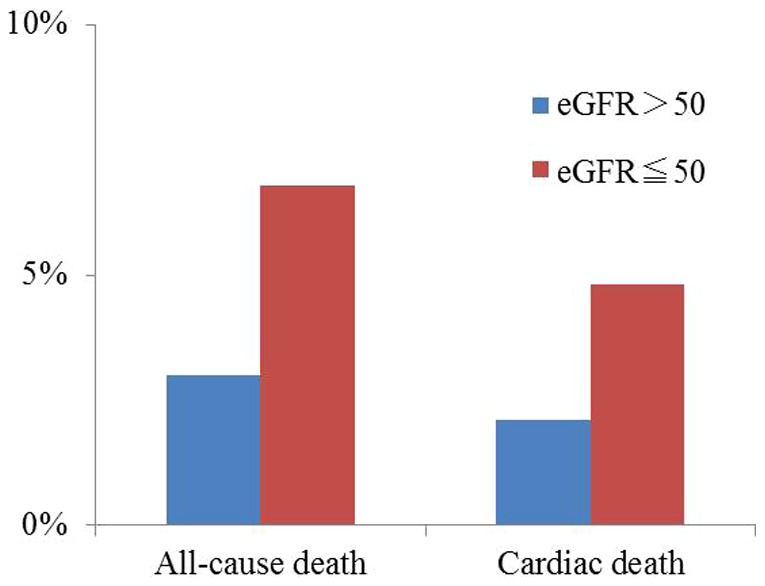
ADHF syndromes registry subjects were evaluated (N = 4,321). Logistic regression modeling calculated adjusted odds ratios (OR) for in-hospital mortality for patients with and without renal dysfunction. Renal dysfunction risk was calculated for subgroups with hypoperfusion-dominant (eg. cold extremities, a low mean blood pressure or a low proportional pulse pressure) or congestion-dominant clinical profiles (eg. peripheral edema, jugular venous distension, or elevated brain natriuretic peptide) to evaluate renal dysfunction's prognostic impact in the context of the two underlying mechanisms. On admission, 2,150 (49.8%) patients aged 73.3 ± 13.6 years had renal dysfunction. Compared with patients without renal dysfunction, those with renal dysfunction were older and had dominant ischemic etiology jugular venous distension, more frequent cold extremities, and higher brain natriuretic peptide levels. Renal dysfunction was associated with in-hospital mortality (OR 2.36; 95% confidence interval 1.75-3.18, p<0.001), and the prognostic impact of renal dysfunction was similar in subgroup of patients with hypoperfusion- or congestion-dominant clinical profiles (p-value for the interaction ranged from 0.104-0.924, and was always >0.05).
Baseline renal dysfunction was significantly associated with in-hospital mortality in ADHF patients. The prognostic impact of renal dysfunction was the same, regardless of its underlying etiologic mechanism.
与急性失代偿性心力衰竭(ADHF)相关的肾功能不全与不良预后相关。其机制归因于肾动脉灌注不足或静脉淤血,但其基于这些临床特征各自的预后影响尚需阐明。
对ADHF综合征登记受试者进行评估(N = 4321)。逻辑回归模型计算了有或无肾功能不全患者住院死亡率的校正比值比(OR)。计算了以灌注不足为主(如四肢冰冷、平均血压低或脉压比例低)或淤血为主的临床特征(如外周水肿、颈静脉扩张或脑钠肽升高)亚组的肾功能不全风险,以评估在两种潜在机制背景下肾功能不全的预后影响。入院时,2150名(49.8%)年龄为73.3±13.6岁的患者存在肾功能不全。与无肾功能不全的患者相比,有肾功能不全的患者年龄更大,主要病因是缺血性,有颈静脉扩张、四肢冰冷更频繁,且脑钠肽水平更高。肾功能不全与住院死亡率相关(OR 2.36;95%置信区间1.75 - 3.18,p<0.001),在以灌注不足或淤血为主的临床特征亚组中,肾功能不全的预后影响相似(交互作用的p值范围为0.104 - 0.924,且始终>0.05)。
基线肾功能不全与ADHF患者的住院死亡率显著相关。无论其潜在病因机制如何,肾功能不全的预后影响相同。