Sliwa Karen, Libhaber Elena, Elliott Catherine, Momberg Zoe, Osman Ayesha, Zühlke Liesl, Lachmann Tony, Nicholson Lauren, Thienemann Friedrich, Roos-Hesselink Jolien, Anthony John
Department of Medicine, Faculty of Health Sciences, Hatter Institute for Cardiovascular Research in Africa, University of Cape Town, Cape Town, South Africa Faculty of Health Sciences, Inter-Cape Heart MRC Unit and Institute of Infectious Diseases and Molecular Medicine, University of Cape Town, Cape Town, South Africa Division of Cardiology, Department of Medicine, Groote Schuur Hospital, University of Cape Town, Cape Town, South Africa Faculty of Health Sciences, School of Clinical Medicine, University of the Witwatersrand, Johannesburg, South Africa.
Faculty of Health Sciences, School of Clinical Medicine, University of the Witwatersrand, Johannesburg, South Africa.
Heart. 2014 Dec;100(24):1967-74. doi: 10.1136/heartjnl-2014-306199. Epub 2014 Sep 16.
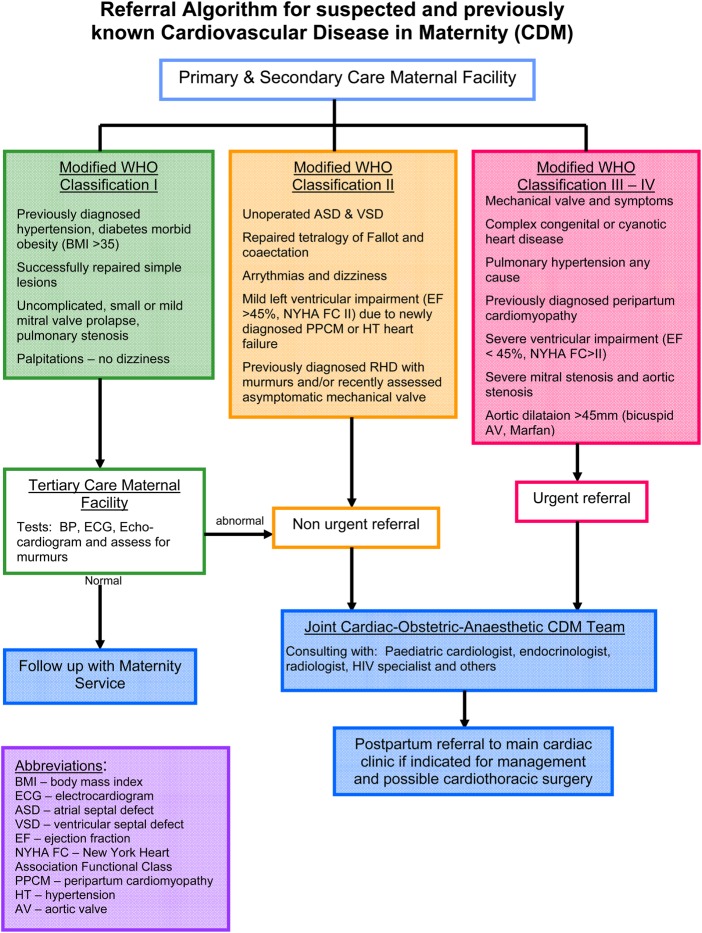
Lack of evidence-based data on the spectrum of cardiovascular disease (CVD) in pregnancy or in the postpartum period, as well as on maternal and fetal outcome, provides challenges for treating physicians, particularly in areas of low resources. The objectives of this study were to investigate the spectrum of disease, mode of presentation and maternal and fetal outcome of patients referred to a dedicated Cardiac Disease and Maternity Clinic (CDM).
The prospective cohort study was conducted at a single tertiary care centre in South Africa. Two hundred and twenty-five women presenting with CVD in pregnancy, or within 6 months postpartum, were studied over a period of 2 years. Clinical assessment, echocardiography and laboratory tests were performed at baseline and follow-up visits. Prepartum, peripartum and postpartum complications were grouped into cardiac, neonatal and obstetric events.
Ethnicity was black African (45%), mixed ethnicity (32%), white (15%), Indian/others (8%) and 12% were HIV positive. Of the 225 consecutive women (mean age 28.8±6.4), 196 (86.7%) presented prepartum and 73 in modified WHO class I. The 152 women presenting in a higher risk group (modified WHO class II-IV) were offered close follow-up at the CDM clinic and were diagnosed with congenital heart disease (32%, 15 operated previously), valvular heart disease (26%, 15 operated previously), cardiomyopathy (27%) and other (15%). Women presenting with symptoms of CVD or heart failure postpartum (n=30) presented in a higher New York Heart Association, had higher heart rates (p<0.001) and NTproBNP levels (p<0.0005). Of the 152 patients, 9 (6%) died within the 6-month follow-up period. Eight of the nine patients died >42 days postpartum. Perinatal death occurred in 1/152 (0.7%)-translating to a perinatal mortality rate of 7/1000 live births.
Disease patterns were markedly different to that seen in the developed world. However, joint obstetric-cardiac care in the low-resource cohort was associated with excellent survival outcome rates of pregnant mothers (even with complex diseases) and their offspring and was similar to that seen in the western world. Mortality typically occurred in the postpartum period, beyond the standard date of recording maternal death.
缺乏关于孕期或产后心血管疾病(CVD)谱以及母婴结局的循证数据,给治疗医生带来了挑战,尤其是在资源匮乏地区。本研究的目的是调查转诊至专门的心脏病与产科诊所(CDM)的患者的疾病谱、表现方式以及母婴结局。
这项前瞻性队列研究在南非的一个单一三级医疗中心进行。对225名在孕期或产后6个月内患有心血管疾病的女性进行了为期2年的研究。在基线和随访时进行了临床评估、超声心动图检查和实验室检查。产前、产时和产后并发症被分为心脏、新生儿和产科事件。
种族为非洲黑人(45%)、混合种族(32%)、白人(15%)、印度人/其他(8%),12%为艾滋病毒阳性。在这225名连续的女性(平均年龄28.8±6.4岁)中,196名(86.7%)在产前就诊,73名属于WHO改良I级。152名就诊于高危组(WHO改良II-IV级)的女性在CDM诊所接受密切随访,被诊断为先天性心脏病(32%,其中15名曾接受手术)、瓣膜性心脏病(26%,其中15名曾接受手术)、心肌病(27%)和其他疾病(15%)。产后出现心血管疾病或心力衰竭症状的女性(n = 30)纽约心脏协会分级更高,心率更高(p<0.001),NTproBNP水平更高(p<0.0005)。在152名患者中,9名(6%)在6个月的随访期内死亡。9名患者中有8名在产后>42天死亡。围产期死亡发生在1/152(0.7%),相当于围产儿死亡率为7/1000活产。
疾病模式与发达国家明显不同。然而,资源匮乏队列中的联合产科-心脏护理与怀孕母亲(即使患有复杂疾病)及其后代的优异生存结局率相关,与西方世界相似。死亡通常发生在产后时期,超出了记录孕产妇死亡的标准日期。