Ndhlovu Lishomwa C, Umaki Tracie, Chew Glen M, Chow Dominic C, Agsalda Melissa, Kallianpur Kalpana J, Paul Robert, Zhang Guangxiang, Ho Erika, Hanks Nancy, Nakamoto Beau, Shiramizu Bruce T, Shikuma Cecilia M
Hawaii Center for AIDS, University of Hawai'i, 651 Ilalo St, BSB 325C, Honolulu, HI, 96815, USA,
J Neurovirol. 2014 Dec;20(6):571-82. doi: 10.1007/s13365-014-0279-x. Epub 2014 Sep 17.
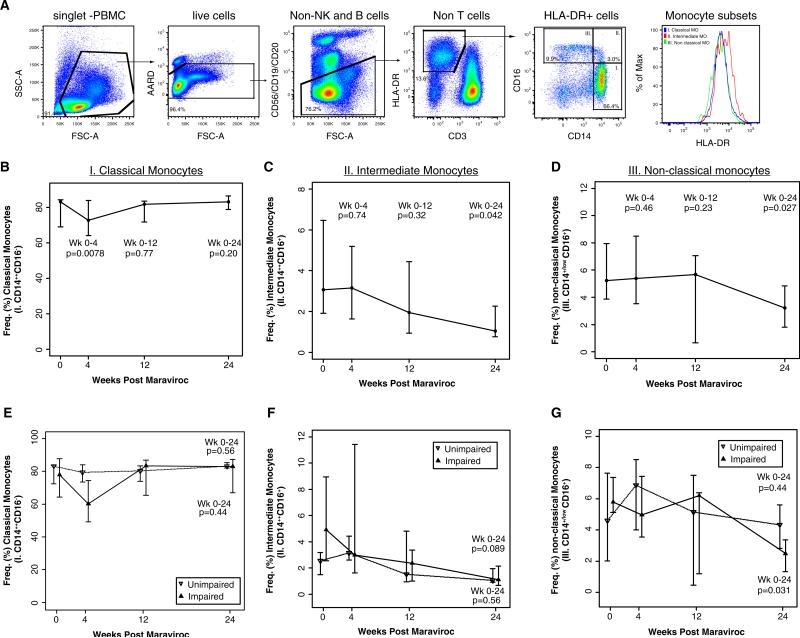
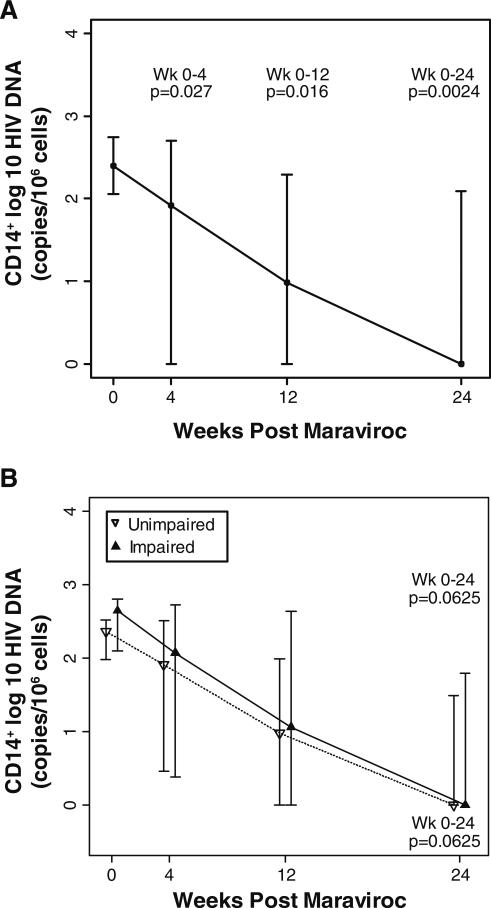
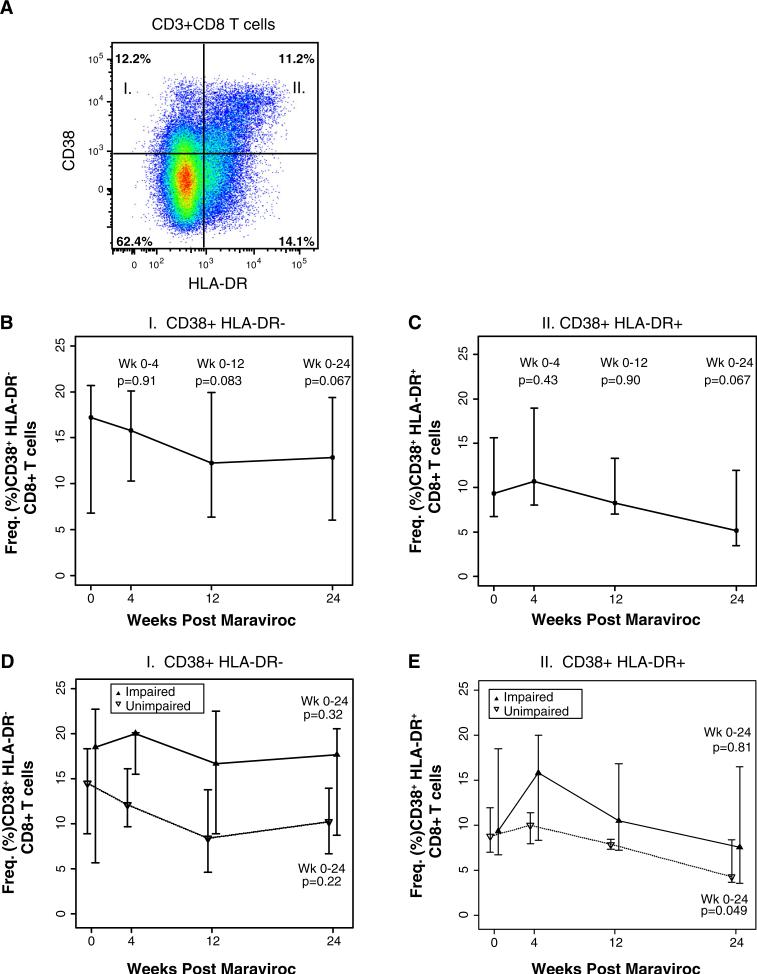
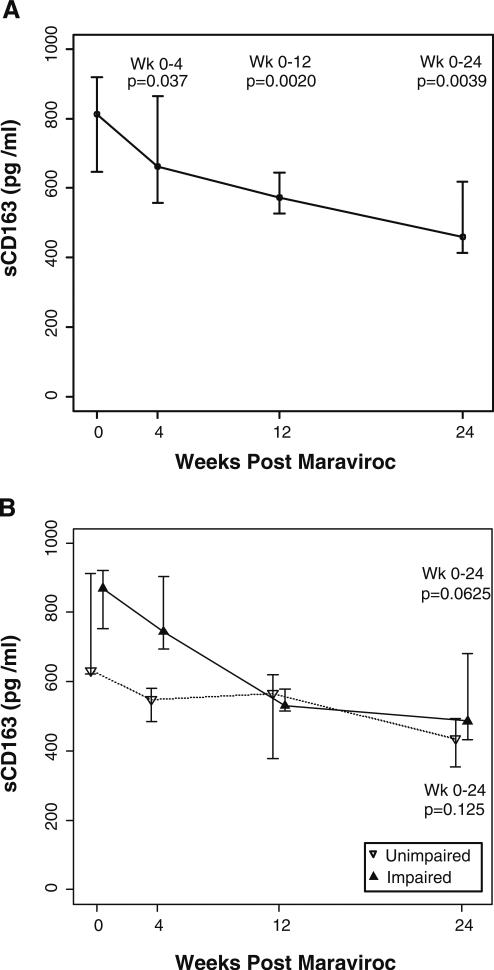
HIV-associated neurocognitive disorders (HAND) continues to be prevalent (30-50%) despite plasma HIV-RNA suppression with combination antiretroviral therapy (cART). There is no proven therapy for individuals on suppressive cART with HAND. We have shown that the degree of HIV reservoir burden (HIV DNA) in monocytes appear to be linked to cognitive outcomes. HIV infection of monocytes may therefore be critical in the pathogenesis of HAND. A single arm, open-labeled trial was conducted to examine the effect of maraviroc (MVC) intensification on monocyte inflammation and neuropsychological (NP) performance in 15 HIV subjects on stable 6-month cART with undetectable plasma HIV RNA (<48 copies/ml) and detectable monocyte HIV DNA (>10 copies/10(6) cells). MVC was added to their existing cART regimen for 24 weeks. Post-intensification change in monocytes was assessed using multiparametric flow cytometry, monocyte HIV DNA content by PCR, soluble CD163 (sCD163) by an ELISA, and NP performance over 24 weeks. In 12 evaluable subjects, MVC intensification resulted in a decreased proportion of circulating intermediate (median; 3.06% (1.93, 6.45) to 1.05% (0.77, 2.26)) and nonclassical (5.2% (3.8, 7.9) to 3.2% (1.8, 4.8)) CD16-expressing monocytes, a reduction in monocyte HIV DNA content to zero log10 copies/10(6) cells and in levels of sCD163 of 43% by 24 weeks. This was associated with significant improvement in NP performance among six subjects who entered the study with evidence of mild to moderate cognitive impairment. The results of this study suggest that antiretroviral therapy with potency against monocytes may have efficacy against HAND.
尽管联合抗逆转录病毒疗法(cART)可抑制血浆HIV-RNA,但HIV相关神经认知障碍(HAND)仍然普遍存在(30%-50%)。对于接受抑制性cART治疗的HAND患者,尚无经证实有效的治疗方法。我们已经表明,单核细胞中HIV储存库负担(HIV DNA)的程度似乎与认知结果有关。因此,单核细胞的HIV感染可能在HAND的发病机制中起关键作用。我们进行了一项单臂、开放标签试验,以研究在15名接受稳定6个月cART治疗、血浆HIV RNA检测不到(<48拷贝/ml)且单核细胞HIV DNA可检测到(>10拷贝/10⁶细胞)的HIV患者中,马拉维若(MVC)强化治疗对单核细胞炎症和神经心理学(NP)表现的影响。将MVC添加到他们现有的cART方案中,持续24周。使用多参数流式细胞术评估强化治疗后单核细胞的变化,通过PCR检测单核细胞HIV DNA含量,通过ELISA检测可溶性CD163(sCD163),并评估24周内的NP表现。在12名可评估的受试者中,MVC强化治疗导致循环中表达CD16的中间型单核细胞(中位数;3.06%(1.93,6.45)降至1.05%(0.77,2.26))和非经典型单核细胞(5.2%(3.8,7.9)降至3.2%(1.8,4.8))的比例降低,单核细胞HIV DNA含量降至零log₁₀拷贝/10⁶细胞,sCD163水平在24周时降低43%。这与6名入组时存在轻度至中度认知障碍证据的受试者的NP表现显著改善相关。这项研究的结果表明,对单核细胞有效的抗逆转录病毒疗法可能对HAND有效。