Zhou Yu-Fen, Xu Ling-Xiao, Huang Li-Ya, Guo Fang, Zhang Fan, He Xiang-Yi, Yuan Yao-Zong, Yao Wei-Yan
Department of Gastroenterology, Ruijin Hospital Affiliated to Shanghai Jiaotong University School of Medicine, Shanghai, P.R. China.
Department of Gastroenterology, General Hospital of Ningxia Medical University, Yinchuan, Ningxia, P.R. China.
Oncol Lett. 2014 Nov;8(5):2096-2102. doi: 10.3892/ol.2014.2429. Epub 2014 Aug 8.
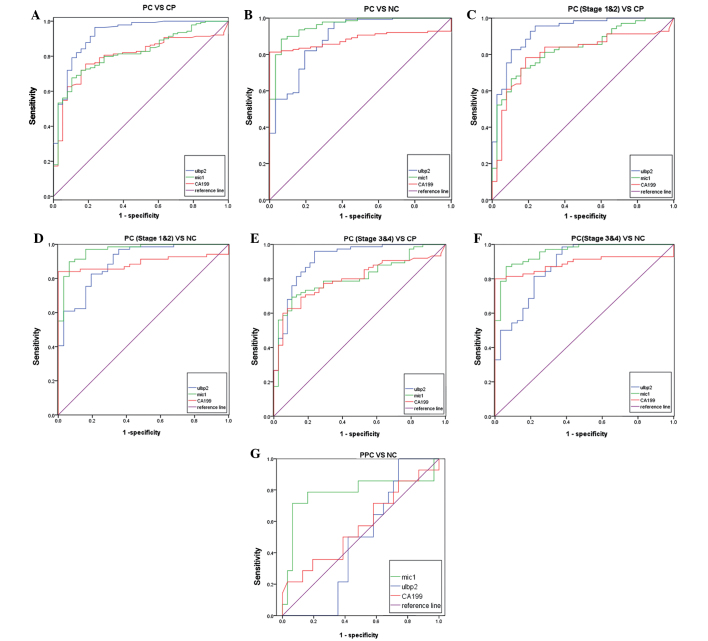
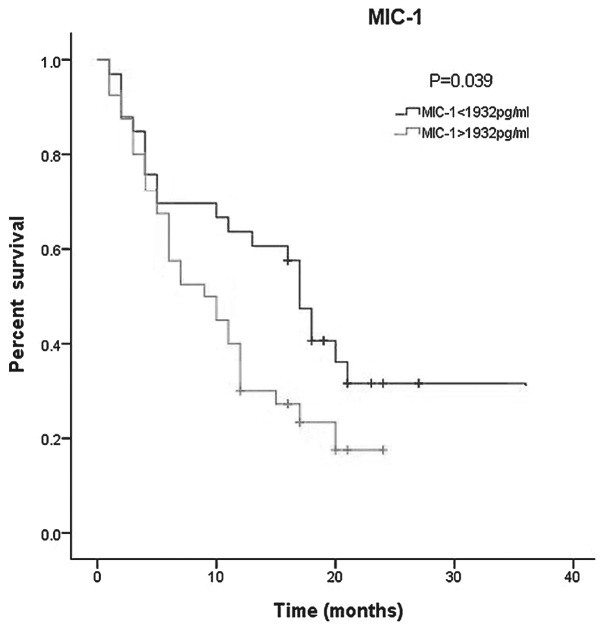
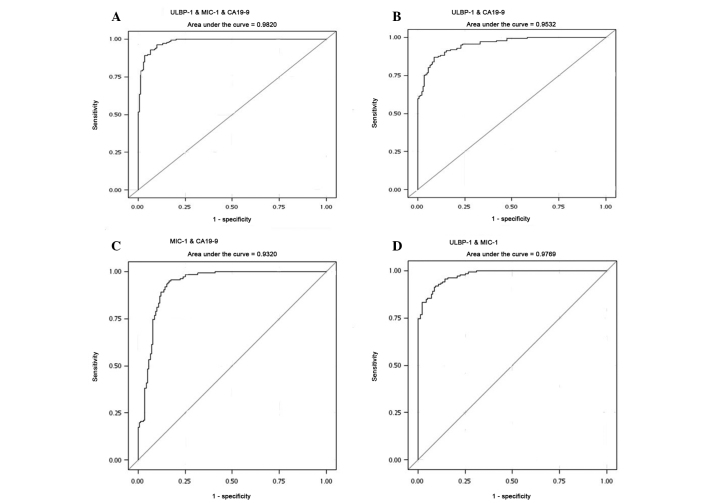
Pancreatic cancer (PC) is the fourth leading cause of cancer-related mortality in the United States. There is no effective serum biomarker for the early diagnosis of PC at present. Although serum UL16-binding protein 2 (ULBP2) and macrophage inhibitory cytokine-1 (MIC-1) levels are reported to be elevated in PC patients, the diagnostic and prognostic value of ULBP2 and MIC-1 alone or in combination remains unknown. The aim of the present case-control study was to compare the diagnostic value of ULBP2, MIC-1 and carbohydrate antigen 19-9 (CA19-9) in 359 serum samples, consisting of 152 cases of PC, 20 cases of pre-pancreatic cancer, 91 cases of chronic pancreatitis (CP) and 96 normal controls (NC). All patients were followed up for a median of 2 years. It was found that the serum levels of ULBP2, MIC-1 and CA19-9 were significantly higher in the PC patients compared with those in the NC group. In distinguishing PC from the CP, the highest sensitivity and specificity were ULBP2 (0.878) and CA19-9 (0.816), respectively. The area under the receiver operating characteristic curve of ULBP2 was 0.923, which was the highest of the three biomarkers. MIC-1 was the optimal choice for the diagnosis of early-stage PC (area under the curve, 0.831). Overall, MIC-1 in combination with ULBP2 improved the diagnostic accuracy in differentiating PC from CP and NC. In addition, a higher level of MIC-1 was correlated with a poorer prognosis, as calculated by the Kaplan-Meier test (P=0.039). Patients with serum MIC-1 levels of ≥1,932 ng/ml had a median survival time of 15.62±2.44 months (mean ± standard deviation) vs. 18.66±2.43 months in patients with a lower level of MIC-1. Overall, combined detection of serum MIC-1 and ULBP2 improved the diagnostic accuracy in differentiating PC from CP and NC, and serum MIC-1 level alone was a predictor of survival in the patients with PC.
胰腺癌(PC)是美国癌症相关死亡的第四大主要原因。目前尚无用于PC早期诊断的有效血清生物标志物。尽管据报道PC患者血清中UL16结合蛋白2(ULBP2)和巨噬细胞抑制细胞因子1(MIC-1)水平升高,但ULBP2和MIC-1单独或联合使用的诊断和预后价值仍不清楚。本病例对照研究的目的是比较ULBP2、MIC-1和糖类抗原19-9(CA19-9)在359份血清样本中的诊断价值,这些样本包括152例PC患者、20例胰腺癌前期患者、91例慢性胰腺炎(CP)患者和96例正常对照(NC)。所有患者均接受了中位时间为2年的随访。结果发现,与NC组相比,PC患者血清中ULBP2、MIC-1和CA19-9水平显著更高。在区分PC与CP时,最高敏感性和特异性分别为ULBP2(0.878)和CA19-9(0.816)。ULBP2的受试者工作特征曲线下面积为0.923,是三种生物标志物中最高的。MIC-1是早期PC诊断的最佳选择(曲线下面积,0.831)。总体而言,MIC-1与ULBP2联合使用提高了区分PC与CP和NC的诊断准确性。此外,通过Kaplan-Meier检验计算,较高水平的MIC-1与较差的预后相关(P=0.039)。血清MIC-1水平≥1932 ng/ml的患者中位生存时间为15.62±2.44个月(均值±标准差),而MIC-1水平较低的患者为18.66±2.43个月。总体而言,血清MIC-1和ULBP2联合检测提高了区分PC与CP和NC的诊断准确性,且单独血清MIC-1水平是PC患者生存的预测指标。