Liu Sandy Z, Staats Paul N, Goicochea Lindsay, Alexiev Borislav A, Shah Nirav, Dixon Renee, Burke Allen P
From the Departments of Pathology and Internal Medicine, University of Maryland, 22 S, Greene St, Baltimore 21201, USA.
Diagn Pathol. 2014 Oct 16;9:174. doi: 10.1186/s13000-014-0174-z.
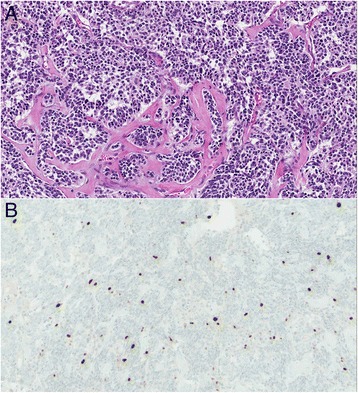
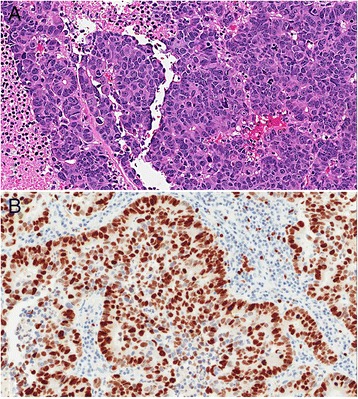
The histopathologic distinction between typical carcinoid (TC) and atypical carcinoid (AC) of the lung is based largely on mitotic index. Ki-67 may aid in separation of these tumors, as well as the distinction from large cell neuroendocrine carcinoma (LCNEC).
We identified 55 surgically resected primary neuroendocrine lung tumors (39 TC, 7 AC, 9 LCNEC) based on mitotic rate and histologic features. Ki-67 proliferative index based on automated image analysis, tumor necrosis, nodal metastases, local or distant recurrence, and survival were compared across groups.
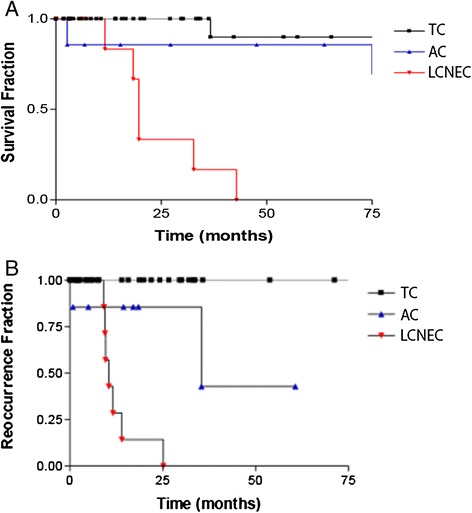
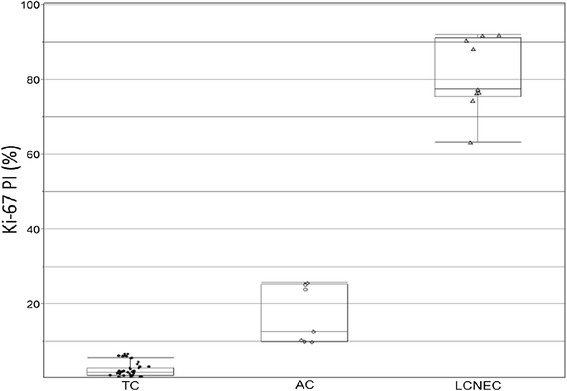
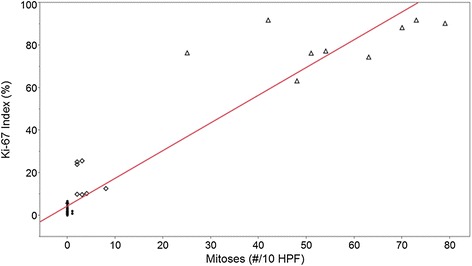
The mean mitotic count and Ki-67 index for TC, AC, and LCNEC were 0.1 and 2.3%, 3.4 and 16.8%, and 56.1 and 81.3% respectively. The Ki-67 index did not overlap among groups, with ranges of 0-6.7% for TC, 9.9-25.7% for AC, and 63.2-91.9% for LCNEC. Nodal metastases were identified in 4/39 (10%) TC, 2/7 (22%) AC, and 2/8 (25%) LCNEC. There was no survival difference between TC and AC, but there was a significant survival difference between LCNEC and TC and AC combined (p<0.001). There was a step-wise increase in disease free survival with tumor grade: no TC recurred, 2/7 AC recurred or progressed (median interval 35.5 months), and all LCNEC recurred or progressed (median interval 10.1 months). No patient with TC or AC died of disease, compared to 7/8 LCNEC with follow-up data.
We conclude that Ki-67 index is a useful diagnostic marker for neuroendocrine tumors, with 7% a divider between AC and TC, and 50% a divider between LCNEC and AC. LCNEC is biologically different from AC and TC, with a much more aggressive course, and a high Ki-67 index.
The virtual slide(s) for this article can be found here: http://www.diagnosticpathology.diagnomx.eu/vs/13000_2014_174.
肺典型类癌(TC)与非典型类癌(AC)的组织病理学区分主要基于有丝分裂指数。Ki-67可能有助于区分这些肿瘤,以及与大细胞神经内分泌癌(LCNEC)相鉴别。
我们根据有丝分裂率和组织学特征,鉴定了55例手术切除的原发性肺神经内分泌肿瘤(39例TC、7例AC、9例LCNEC)。比较了各组基于自动图像分析的Ki-67增殖指数、肿瘤坏死、淋巴结转移、局部或远处复发及生存率。
TC、AC和LCNEC的平均有丝分裂计数及Ki-67指数分别为0.1和2.3%、3.4和16.8%、56.1和81.3%。各组间Ki-67指数无重叠,TC为0-6.7%,AC为9.9-25.7%,LCNEC为63.2-91.9%。4/39(10%)例TC、2/7(22%)例AC及2/8(25%)例LCNEC发现有淋巴结转移。TC和AC之间生存率无差异,但LCNEC与TC和AC联合组之间生存率有显著差异(p<0.001)。随着肿瘤分级的增加,无病生存率呈逐步上升趋势:TC均未复发,2/7例AC复发或进展(中位间隔35.5个月),所有LCNEC均复发或进展(中位间隔10.1个月)。与7/8例有随访数据的LCNEC相比,TC或AC患者均未死于该疾病。
我们得出结论,Ki-67指数是神经内分泌肿瘤的一种有用诊断标志物,7%是AC与TC的分界值,50%是LCNEC与AC的分界值。LCNEC在生物学上与AC和TC不同,病程更具侵袭性,且Ki-67指数较高。
本文的虚拟切片可在此处找到:http://www.diagnosticpathology.diagnomx.eu/vs/13000_2014_174。