Ki Myung, Baek Sujin, Yun Young-duk, Kim Namhoon, Hyde Martin, Na Baegju
Department of Preventive Medicine, College of Medicine, Konyang University, Konyang Univ, Gwanjeo Campus, Gasuwon-dong, Seo-gu, Daejeon 302-833, Korea.
BMC Geriatr. 2014 Oct 16;14:111. doi: 10.1186/1471-2318-14-111.
Age-related differences in diabetes outcomes are important both for clinical and policy considerations. To clarify the basis of such differences, we investigated patterns of associations for age in relation to hospitalization and glycemic control and examined the role of other factors.
4471 patients with diabetes aged 40-79 years were drawn from a retrospectively retrieved National Health Insurance Cohort. Using logistic regression, risk factors measured over the two years (2007-2008) were examined for their associations with hospitalization and poor glycemic control during the last year (2009) of follow-up.
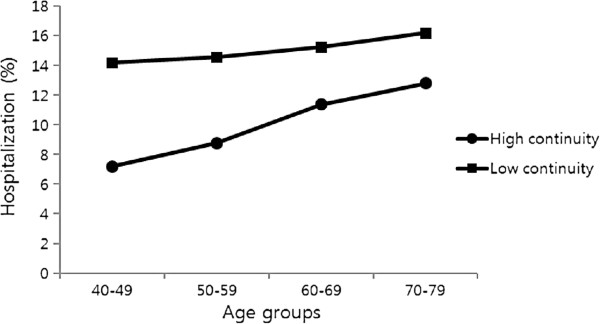
Compared to the middle-aged patients, older patients were more likely to have been hospitalized (Adjusted odds ratio (OR(adjusted)) = 1.97(95% CI = 1.28, 3.04) for the oldest group (ages 70-79) vs youngest group (ages 40-49)) but less likely to have poor glycemic control (OR(adjusted) = 0.45 (95% CI = 0.37, 0.56) for the oldest group vs youngest group). Older patients were also less likely to be obese but had more complications, longer duration of diabetes, lower continuity of care, and higher blood pressure and total cholesterol level. The pattern of associations for hospitalization and glycemic control was not uniform across the risk factors, sharing only a few common factors such as the duration of diabetes and blood pressure. In general, poor glycemic control was affected predominantly by metabolic management, while hospitalization was strongly related to functional status (i.e., number of complications) and care quality measures (i.e., continuity of care).
Hospitalization was higher among the older diabetic patients, despite better glycemic control. Factors were differently associated with the two diabetes-related outcomes, providing more comprehensive risk profiles for hospitalization. The co-existence of improved glycemic control and increased hospitalization among older diabetic patients suggests an extension of a geriatric evaluation to wider functional and comorbidity status.
糖尿病结局的年龄相关差异对于临床和政策考量均具有重要意义。为阐明此类差异的基础,我们研究了年龄与住院治疗及血糖控制之间的关联模式,并考察了其他因素的作用。
从回顾性获取的国民健康保险队列中选取了4471例年龄在40 - 79岁的糖尿病患者。运用逻辑回归分析,对在两年(2007 - 2008年)期间测量的风险因素与随访最后一年(2009年)的住院治疗及血糖控制不佳之间的关联进行了考察。
与中年患者相比,老年患者住院的可能性更高(最年长组(70 - 79岁)与最年轻组(40 - 49岁)相比,调整后的优势比(OR(调整))= 1.97(95%置信区间 = 1.28, 3.04)),但血糖控制不佳的可能性更低(最年长组与最年轻组相比,OR(调整) = 0.45(95%置信区间 = 0.37, 0.56))。老年患者肥胖的可能性也更低,但并发症更多、糖尿病病程更长、医疗连续性更低,且血压和总胆固醇水平更高。住院治疗和血糖控制的关联模式在各风险因素中并不一致,仅共享少数共同因素,如糖尿病病程和血压。总体而言,血糖控制不佳主要受代谢管理影响,而住院治疗与功能状态(即并发症数量)和医疗质量指标(即医疗连续性)密切相关。
尽管血糖控制较好,但老年糖尿病患者的住院率更高。各因素与两种糖尿病相关结局的关联不同,为住院治疗提供了更全面的风险概况。老年糖尿病患者血糖控制改善与住院率增加并存,提示应将老年评估扩展至更广泛的功能和共病状态。