Hanifi Syed M A, Mahmood Shehrin S, Bhuiya Abbas
INDEPTH Network, Accra, Ghana; Centre for Equity and Health Systems, ICDDR,B, Dhaka, Bangladesh;
INDEPTH Network, Accra, Ghana; Centre for Equity and Health Systems, ICDDR,B, Dhaka, Bangladesh.
Glob Health Action. 2014 Oct 29;7:25473. doi: 10.3402/gha.v7.25473. eCollection 2014.
Bangladesh has achieved remarkable gains in health indicators during the last four decades despite low levels of economic development. However, the persistence of inequities remains disturbing. This success was also accompanied by health and demographic transitions, which in turn brings new challenges for a nation that has yet to come to terms with pre-transition health challenges. It is therefore important to understand the causes of death and their relationship with socioeconomic status (SES).
The paper aims to assess the causes of death by SES based on surveillance data from a rural area of Bangladesh, in order to understand the situation and inform policy makers and programme leaders.
We analysed population-based mortality data collected from the Chakaria Health and Demographic Surveillance System in Bangladesh. The causes of death were determined by using a Bayesian-based programme for interpreting verbal autopsy findings (InterVA-4). The data included 1,391 deaths in 217,167 person-years of observation between 2010 and 2012. The wealth index constructed using household assets was used to assess the SES, and disease burdens were compared among the wealth quintiles.
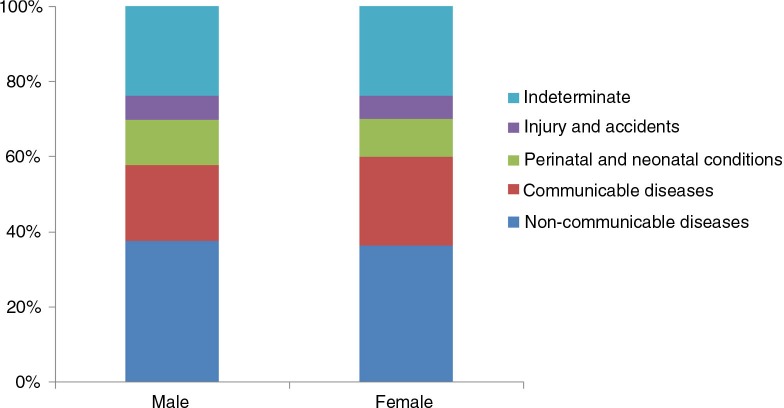
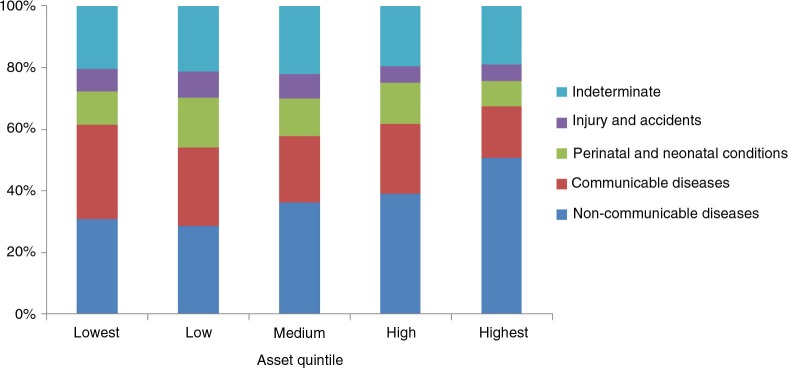
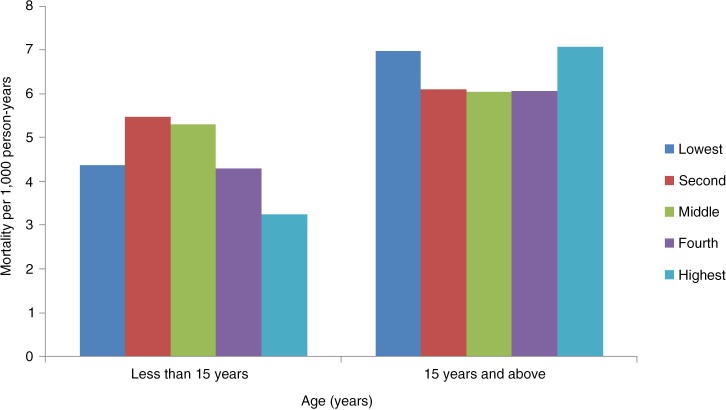
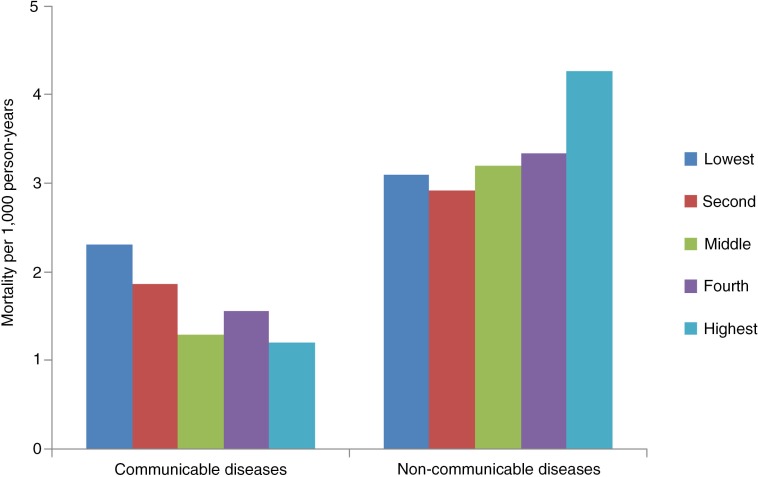
Analysing cause of death (CoD) revealed that non-communicable diseases (NCDs) were the leading causes of deaths (37%), followed by communicable diseases (CDs) (22%), perinatal and neonatal conditions (11%), and injury and accidents (6%); the cause of remaining 24% of deaths could not be determined. Age-specific mortality showed premature birth, respiratory infections, and drowning were the dominant causes of death for childhood mortality (0-14 years), which was inversely associated with SES (p<0.04). For adult and the elderly (15 years and older), NCDs were the leading cause of death (51%), followed by CDs (23%). For adult and the elderly, NCDs concentrated among the population from higher SES groups (p<0.005), and CDs among the lower SES groups (p<0.001).
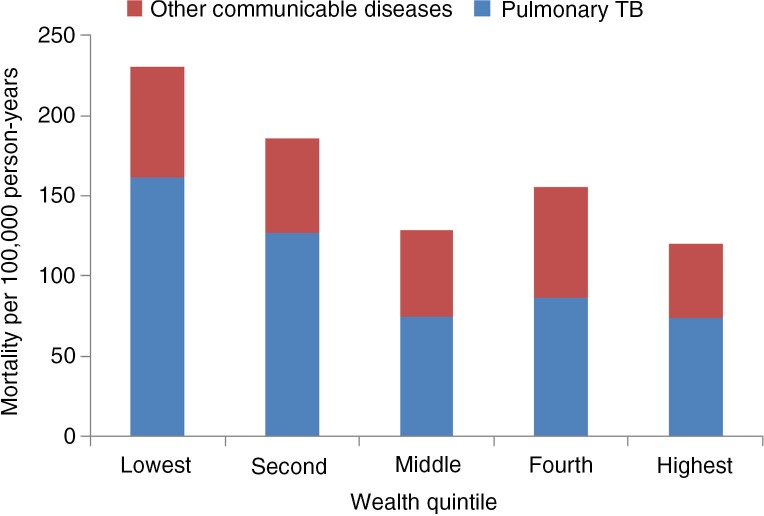
Epidemiologic transition is taking place with a shift from the dominance of CDs to NCDs. SES inequity in mortality still persists--the poor suffer from CDs in all age groups, whereas those better off suffer more from NCDs than CDs. Policy makers thus need to consider the social distribution of diseases before developing any public health action targeted towards reducing mortality and the extent of disease burden in an equitable manner.
尽管经济发展水平较低,但孟加拉国在过去四十年中在健康指标方面取得了显著进展。然而,不平等现象的持续存在仍然令人不安。这一成功还伴随着健康和人口结构转型,这反过来又给一个尚未应对转型前健康挑战的国家带来了新的挑战。因此,了解死亡原因及其与社会经济地位(SES)的关系非常重要。
本文旨在根据孟加拉国农村地区的监测数据,按社会经济地位评估死亡原因,以便了解情况并为政策制定者和项目负责人提供信息。
我们分析了从孟加拉国查卡里亚健康与人口监测系统收集的基于人群的死亡率数据。死亡原因通过使用基于贝叶斯的程序来解释口头尸检结果(InterVA-4)来确定。数据包括2010年至2012年期间217,167人年观察期内的1391例死亡。使用家庭资产构建的财富指数用于评估社会经济地位,并在五个财富五分位数之间比较疾病负担。
对死亡原因(CoD)的分析表明,非传染性疾病(NCDs)是主要死因(37%),其次是传染病(CDs)(22%)、围产期和新生儿疾病(11%)以及伤害和事故(6%);其余24%的死亡原因无法确定。特定年龄死亡率显示,早产、呼吸道感染和溺水是儿童死亡率(0至14岁)的主要死因,这与社会经济地位呈负相关(p<0.04)。对于成年人和老年人(15岁及以上),非传染性疾病是主要死因(51%),其次是传染病(23%)。对于成年人和老年人,非传染性疾病集中在社会经济地位较高的人群中(p<0.005),而传染病集中在社会经济地位较低的人群中(p<0.001)。
正在发生流行病学转型,从传染病占主导地位转向非传染性疾病占主导地位。死亡率方面的社会经济地位不平等仍然存在——穷人在所有年龄组都遭受传染病困扰,而富裕人群患非传染性疾病的情况比传染病更严重。因此,政策制定者在制定任何旨在以公平方式降低死亡率和疾病负担程度的公共卫生行动之前,需要考虑疾病的社会分布情况。