Cooper Alicia L, Dore David D, Kazis Lewis E, Mor Vincent, Trivedi Amal N
Department of Health Services, Policy and Practice, Brown University, Box G-S121-6, Providence, RI 02912. E-mail:
Am J Manag Care. 2014 Oct 1;20(10):e469-78.
To examine patient, community, and insurance plan predictors of high-risk prescribing in the elderly Medicare Advantage population.
Cohort study.
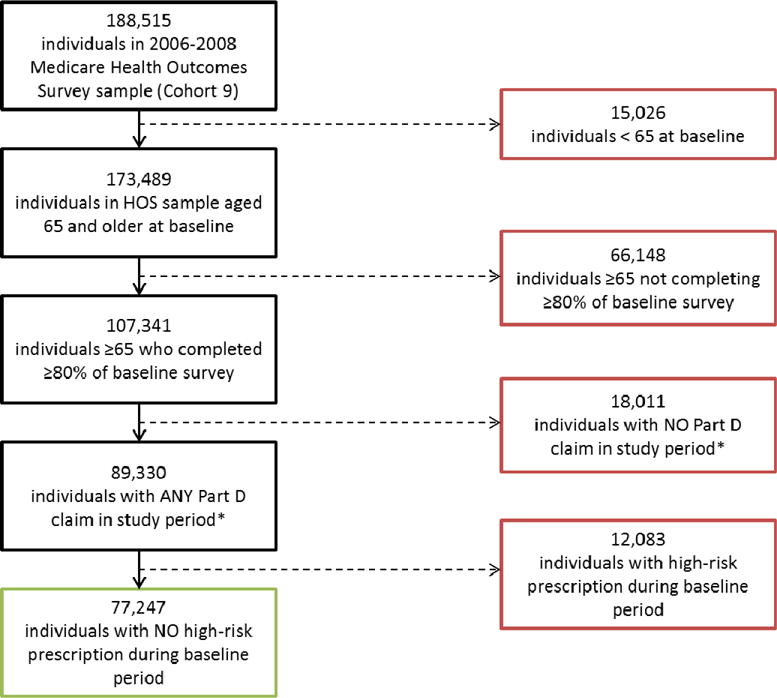
Using a sample of 203 Medicare Advantage plans from the 2006-2008 Health Outcomes Survey, we compared patient, community, and insurance plan characteristics of 77,247 respondents with and without new Medicare Part D claims for high-risk medications from June 2006 to May 2007.
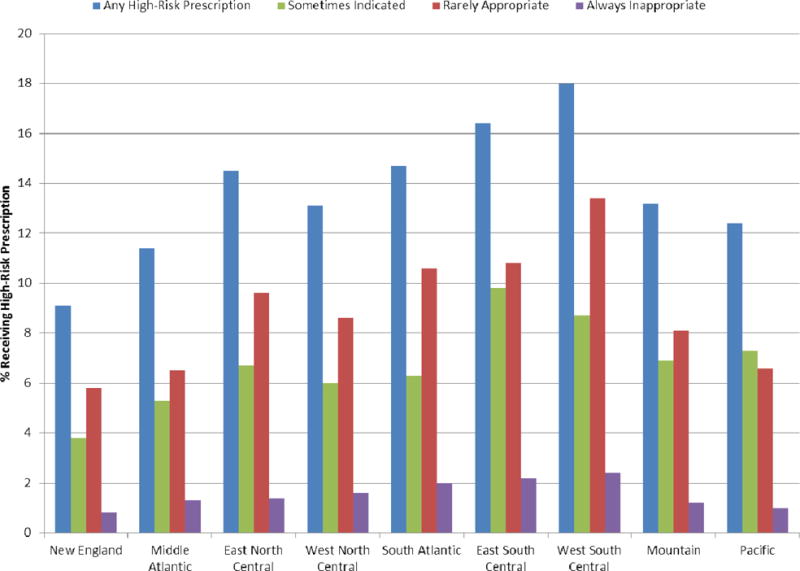
Of the Medicare Advantage enrollee respondents, 15.6% received a new prescription for a high-risk medication during 12 months of follow-up. In adjusted analyses, new users of high-risk medications were more likely to be women (OR = 1.35; 95% CI,1.28-1.42), and they reported poorer general health (Physical Component Summary score 37.3 vs 40.4, P <.05) than did individuals who never received a high-risk prescription. Being aged ≥ 85 years was protective against receipt of a high-risk medication (OR relative to persons aged 65-69 years = 0.69; 95% CI, 0.64-0.75). Incidence of high-risk prescribing varied by census division, with a 2-fold difference between regions with the lowest and highest rates (9% in New England vs 18% in the West South Central region). Muscle relaxants, antihistamines, and opiates accounted for over 71% of new dispensing of high-risk medications. Approximately 67% of new users of high-risk medications received only 1 dispensing.
High-risk prescribing varies widely by geography and drug class in the Medicare Advantage population. Women, persons with poorer self-reported health, and those residing in the Southern regions of the United States more frequently receive high-risk medications. Variations may highlight areas for targeted interventions to reduce high-risk prescribing to the elderly.
研究老年医疗保险优势计划人群中高风险处方的患者、社区及保险计划预测因素。
队列研究。
利用2006 - 2008年健康结果调查中的203个医疗保险优势计划样本,比较了2006年6月至2007年5月期间有和没有新的医疗保险D部分高风险药物索赔的77247名受访者的患者、社区及保险计划特征。
在医疗保险优势计划参保受访者中,15.6%在12个月的随访期间收到了高风险药物的新处方。在调整分析中,高风险药物的新使用者更可能是女性(比值比=1.35;95%置信区间,1.28 - 1.42),且与从未收到高风险处方的个体相比,他们报告的总体健康状况较差(身体成分汇总得分37.3对40.4,P<.05)。年龄≥85岁可预防高风险药物的使用(相对于65 - 69岁人群的比值比=0.69;95%置信区间,0.64 - 0.75)。高风险处方的发生率因人口普查区而异,最低和最高发生率地区之间相差2倍(新英格兰地区为9%,而西南中部地区为18%)。肌肉松弛剂、抗组胺药和阿片类药物占高风险药物新配药的71%以上。约67%的高风险药物新使用者仅接受了1次配药。
医疗保险优势计划人群中,高风险处方在地理区域和药物类别上差异很大。女性、自我报告健康状况较差的人以及居住在美国南部地区的人更频繁地接受高风险药物。这些差异可能突出了有针对性干预措施的领域,以减少对老年人的高风险处方。